

Trans-Umbilical Lymphadenectomy Using an Articulating Bipolar Vessel-Sealing Device (TULAB) during Robotic Surgery for Gastric Cancer: Enhancing the Surgeon's Eye for Reduced-Port Robotic Gastrectomy
- PMID: 38001631
- PMCID: PMC10670095
- DOI: 10.3390/cancers15225371
Trans-Umbilical Lymphadenectomy Using an Articulating Bipolar Vessel-Sealing Device (TULAB) during Robotic Surgery for Gastric Cancer: Enhancing the Surgeon's Eye for Reduced-Port Robotic Gastrectomy
Abstract
Background: Docking the scope and instruments through a multi-channel trocar has enabled reduced-port robotic distal gastrectomy (RRDG) for gastric cancer. To facilitate lymphadenectomy over the anatomical hindrances during RRDG, we recently introduced the Vessel Sealer Extend® (VSE) (Intuitive Surgical, Sunnyvale, CA, USA), a bipolar vessel-sealing device (BVSD) with an articulating jaw.
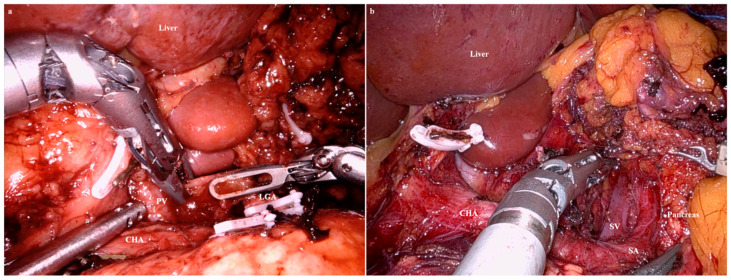
Methods: From May 2020 to August 2023, we performed RRDG to treat T1 gastric cancer. One endoscope arm and three instrument arms of the da Vinci® Xi Surgical System (Intuitive Surgical) were used. During the lymphadenectomy, the endoscope and VSE (Intuitive Surgical) were docked through a multi-channel trocar established on a trans-umbilical incision. Two Cardiere forceps were docked through cannulas established on each flank. A trans-umbilical lymphadenectomy using an articulating BVSD (TULAB) was then performed.
Results: A total of 42 patients underwent planned RRDG with the TULAB technique. The number of retrieved lymph nodes did not differ between the patients who underwent RRDG and those who underwent conventional laparoscopic distal gastrectomies (CLDG) (p = 0.362). There was no statistically significant difference in postoperative complications between the RRDG and CLDG group (p = 0.189). The mean time to first semi-fluid diet was shorter in the patients who underwent RRDG than CLDG (p = 0.030), and the incidence of postoperative ileus was lower in the RRDG group than the CLDG group (0% and 9.9%, respectively, p = 0.034).
Conclusions: Despite use of fewer ports, RRDG with TULAB had similar outcomes to CLDG in terms of the incidence of postoperative morbidity and the number of harvested lymph nodes. Furthermore, by reducing the number of incisions, the incidence of the intra-abdominal adhesions can potentially be lowered when RRDG is used.
Keywords: Vessel Sealer Extend® (VSE); gastric cancer; reduced-port robotic distal gastrectomy (RRDG); trans-umbilical lymphadenectomy using an articulating BVSD (TULAB).
Conflict of interest statement
The authors declare no conflict of interest.
Figures




Similar articles
-
D2 Lymph Node Dissections during Reduced-port Robotic Distal Subtotal Gastrectomy and Conventional Laparoscopic Surgery Performed by a Single Surgeon in a High-volume Center: a Propensity Score-matched Analysis.J Gastric Cancer. 2020 Dec;20(4):431-441. doi: 10.5230/jgc.2020.20.e36. Epub 2020 Dec 24. J Gastric Cancer. 2020. PMID: 33425444 Free PMC article.
-
Lymphadenectomy using two instrument arms during robotic surgery for gastric cancer: A strategy to facilitate reduced-port robotic gastrectomy.Asian J Surg. 2020 Mar;43(3):459-466. doi: 10.1016/j.asjsur.2019.05.014. Epub 2019 Jun 18. Asian J Surg. 2020. PMID: 31227438
-
Safety and feasibility of reduced-port robotic distal gastrectomy for gastric cancer: a phase I/II clinical trial.Surg Endosc. 2017 Oct;31(10):4002-4009. doi: 10.1007/s00464-017-5435-y. Epub 2017 Feb 15. Surg Endosc. 2017. PMID: 28205030 Clinical Trial.
-
Perioperative outcomes of robotic versus laparoscopic distal gastrectomy for gastric cancer: a meta-analysis of propensity score-matched studies and randomized controlled trials.BMC Surg. 2022 Dec 14;22(1):427. doi: 10.1186/s12893-022-01881-9. BMC Surg. 2022. PMID: 36517776 Free PMC article.
-
Current status of robotic gastrectomy for gastric cancer.Surg Today. 2016 May;46(5):528-34. doi: 10.1007/s00595-015-1190-7. Epub 2015 May 28. Surg Today. 2016. PMID: 26019020 Review.
References
-
- Kim H.-I., Han S.-U., Yang H.-K., Kim Y.-W., Lee H.-J., Ryu K.W., Park J.-M., An J.Y., Kim M.-C., Park S., et al. Multicenter Prospective Comparative Study of Robotic Versus Laparoscopic Gastrectomy for Gastric Adenocarcinoma. Ann. Surg. 2016;263:103–109. doi: 10.1097/SLA.0000000000001249. - DOI - PubMed
-
- Suda K., Man I.M., Ishida Y., Kawamura Y., Satoh S., Uyama I. Potential advantages of robotic radical gastrectomy for gastric adenocarcinoma in comparison with conventional laparoscopic approach: A single institutional retrospective comparative cohort study. Surg. Endosc. 2015;29:673–685. doi: 10.1007/s00464-014-3718-0. - DOI - PubMed
-
- Obama K., Kim Y.M., Kang D.R., Son T., Kim H., Noh S.H., Hyung W.J. Long-term oncologic outcomes of robotic gastrectomy for gastric cancer compared with laparoscopic gastrectomy. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2018;21:285–295. doi: 10.1007/s10120-017-0740-7. - DOI - PubMed
-
- Seo W.J., Son T., Roh C.K., Cho M., Kim H.I., Hyung W.J. Reduced-port totally robotic distal subtotal gastrectomy with lymph node dissection for gastric cancer: A modified technique using Single-Site((R)) and two additional ports. Surg. Endosc. 2018;32:3713–3719. doi: 10.1007/s00464-018-6208-y. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
