

Patient Characteristics Associated with Growth of Patient-Derived Tumor Implants in Mice (Patient-Derived Xenografts)
- PMID: 38001663
- PMCID: PMC10670531
- DOI: 10.3390/cancers15225402
Patient Characteristics Associated with Growth of Patient-Derived Tumor Implants in Mice (Patient-Derived Xenografts)
Abstract
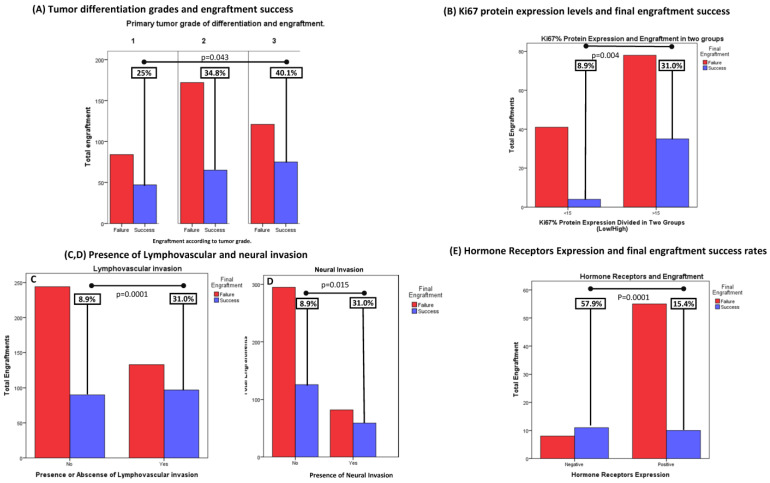
Background: patient-derived xenografts (PDXs) have defined the field of translational cancer research in recent years, becoming one of the most-used tools in early drug development. The process of establishing cancer models in mice has turned out to be challenging, since little research focuses on evaluating which factors impact engraftment success. We sought to determine the clinical, pathological, or molecular factors which may predict better engraftment rates in PDXs. Methods: between March 2017 and January 2021, tumor samples obtained from patients with primary or metastatic cancer were implanted into athymic nude mice. A full comprehensive evaluation of baseline factors associated with the patients and patients' tumors was performed, with the goal of potentially identifying predictive markers of engraftment. We focused on clinical (patient factors) pathological (patients' tumor samples) and molecular (patients' tumor samples) characteristics, analyzed either by immunohistochemistry (IHC) or next-generation sequencing (NGS), which were associated with the likelihood of final engraftment, as well as with tumor growth rates in xenografts. Results: a total of 585 tumor samples were collected and implanted. Twenty-one failed to engraft, due to lack of malignant cells. Of 564 tumor-positive samples, 187 (33.2%) grew at time of analysis. The study was able to find correlation and predictive value for engraftment for the following: the use of systemic antibiotics by the patient within 2 weeks of sampling (38.1% (72/189) antibiotics- group vs. 30.7% (115/375) no-antibiotics) (p = 0.048), and the administration of systemic steroids to the patients within 2 weeks of sampling (41.5% (34/48) steroids vs. 31.7% (153/329), no-steroids) (p = 0.049). Regarding patient's baseline tests, we found certain markers could help predict final engraftment success: for lactate dehydrogenase (LDH) levels, 34.1% (140/411) of tumors derived from patients with baseline blood LDH levels above the upper limit of normality (ULN) achieved growth, against 30.7% (47/153) with normal LDH (p = 0.047). Histological tumor characteristics, such as grade of differentiation, were also correlated. Grade 1: 25.4% (47/187), grade 2: 34.8% (65/187) and grade 3: 40.1% (75/187) tumors achieved successful growth (p = 0.043), suggesting the higher the grade, the higher the likelihood of success. Similarly, higher ki67 levels were also correlated with better engraftment rates: low (Ki67 < 15%): 8.9% (9/45) achieved growth vs. high (Ki67 ≥ 15%): 31% (35/113) (p: 0.002). Other markers of aggressiveness such as the presence of lymphovascular invasion in tumor sample of origin was also predictive: 42.2% (97/230) with lymphovascular vs. 26.9% (90/334) of samples with no invasion (p = 0.0001). From the molecular standpoint, mismatch-repair-deficient (MMRd) tumors showed better engraftment rates: 62.1% (18/29) achieved growth vs. 40.8% (75/184) of proficient tumors (p = 0.026). A total of 84 PDX were breast models, among which 57.9% (11/19) ER-negative models grew, vs. 15.4% (10/65) of ER-positive models (p = 0.0001), also consonant with ER-negative tumors being more aggressive. BRAFmut cancers are more likely to achieve engraftment during the development of PDX models. Lastly, tumor growth rates during first passages can help establish a cutoff point for the decision-making process during PDX development, since the higher the tumor grades, the higher the likelihood of success. Conclusions: tumors with higher grade and Ki67 protein expression, lymphovascular and/or perineural invasion, with dMMR and are negative for ER expression have a higher probability of achieving growth in the process of PDX development. The use of steroids and/or antibiotics in the patient prior to sampling can also impact the likelihood of success in PDX development. Lastly, establishing a cutoff point for tumor growth rates could guide the decision-making process during PDX development.
Keywords: PDX; cancer; engraftment; mice; models; oncology; patient-derived xenografts; preclinical; prediction; translational; tumor growth.
Conflict of interest statement
There are no competing interests to be disclosed for any of the authors regarding this work.
Figures





References
-
- Hidalgo M., Amant F., Biankin A.V., Budinská E., Byrne A.T., Caldas C., Clarke R.B., de Jong S., Jonkers J., Mælandsmo G.M., et al. Patient-Derived Xenograft Models: An Emerging Platform for Translational Cancer Research. Cancer Discov. 2014;4:998–1013. doi: 10.1158/2159-8290.CD-14-0001. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
