

A Systematic Review of Deep-Learning Methods for Intracranial Aneurysm Detection in CT Angiography
- PMID: 38001922
- PMCID: PMC10669551
- DOI: 10.3390/biomedicines11112921
A Systematic Review of Deep-Learning Methods for Intracranial Aneurysm Detection in CT Angiography
Abstract
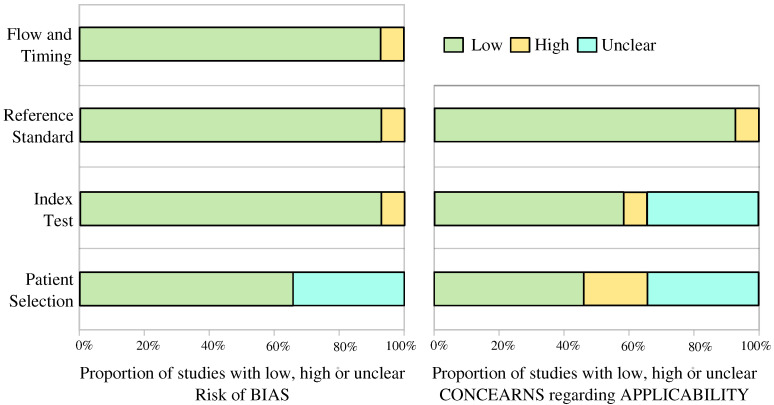
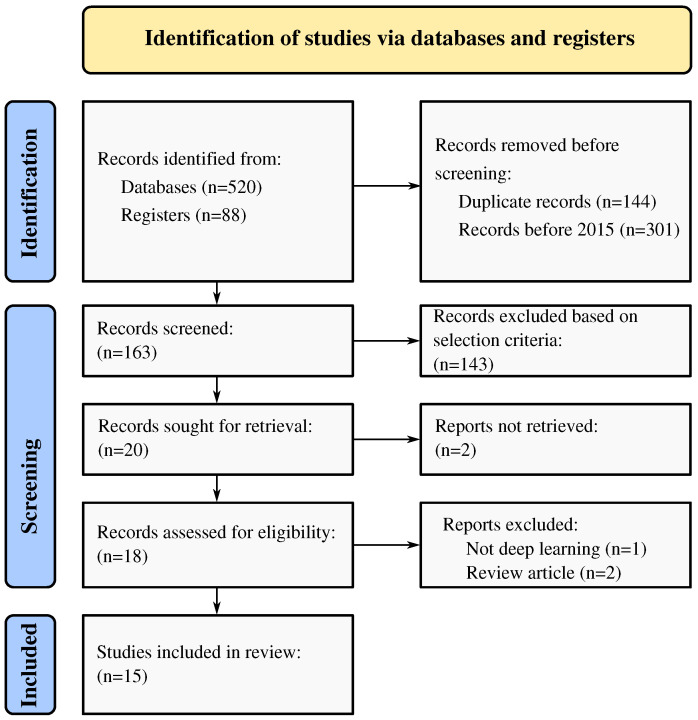
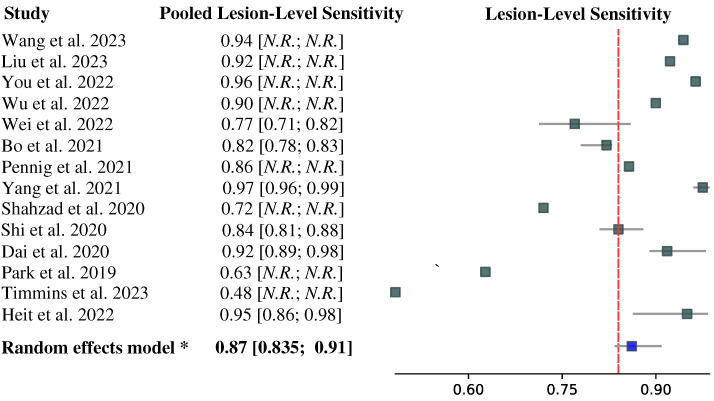
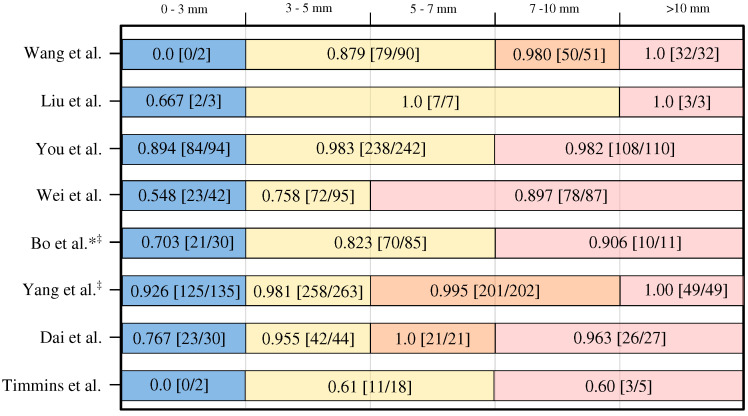
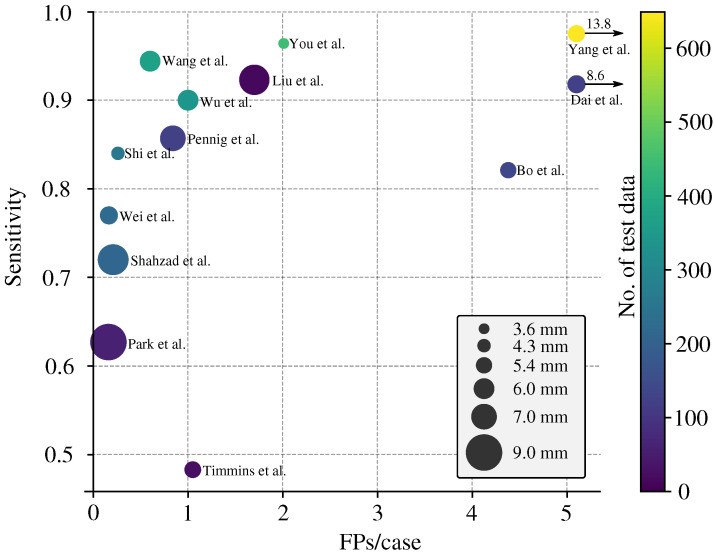
Background: Subarachnoid hemorrhage resulting from cerebral aneurysm rupture is a significant cause of morbidity and mortality. Early identification of aneurysms on Computed Tomography Angiography (CTA), a frequently used modality for this purpose, is crucial, and artificial intelligence (AI)-based algorithms can improve the detection rate and minimize the intra- and inter-rater variability. Thus, a systematic review and meta-analysis were conducted to assess the diagnostic accuracy of deep-learning-based AI algorithms in detecting cerebral aneurysms using CTA. Methods: PubMed (MEDLINE), Embase, and the Cochrane Library were searched from January 2015 to July 2023. Eligibility criteria involved studies using fully automated and semi-automatic deep-learning algorithms for detecting cerebral aneurysms on the CTA modality. Eligible studies were assessed using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines and the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) tool. A diagnostic accuracy meta-analysis was conducted to estimate pooled lesion-level sensitivity, size-dependent lesion-level sensitivity, patient-level specificity, and the number of false positives per image. An enhanced FROC curve was utilized to facilitate comparisons between the studies. Results: Fifteen eligible studies were assessed. The findings indicated that the methods exhibited high pooled sensitivity (0.87, 95% confidence interval: 0.835 to 0.91) in detecting intracranial aneurysms at the lesion level. Patient-level sensitivity was not reported due to the lack of a unified patient-level sensitivity definition. Only five studies involved a control group (healthy subjects), whereas two provided information on detection specificity. Moreover, the analysis of size-dependent sensitivity reported in eight studies revealed that the average sensitivity for small aneurysms (<3 mm) was rather low (0.56). Conclusions: The studies included in the analysis exhibited a high level of accuracy in detecting intracranial aneurysms larger than 3 mm in size. Nonetheless, there is a notable gap that necessitates increased attention and research focus on the detection of smaller aneurysms, the use of a common test dataset, and an evaluation of a consistent set of performance metrics.
Keywords: CTA; PRISMA; QUADAS-2; aneurysm detection; computed tomography angiography; evaluation guidelines; false positives per image; healthy controls; meta-analysis; sensitivity; specificity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Detection of cerebral aneurysms using artificial intelligence: a systematic review and meta-analysis.J Neurointerv Surg. 2023 Mar;15(3):262-271. doi: 10.1136/jnis-2022-019456. Epub 2022 Nov 14. J Neurointerv Surg. 2023. PMID: 36375834 Free PMC article.
-
Deep Learning for Detection of Intracranial Aneurysms from Computed Tomography Angiography Images.J Digit Imaging. 2023 Feb;36(1):114-123. doi: 10.1007/s10278-022-00698-5. Epub 2022 Sep 9. J Digit Imaging. 2023. PMID: 36085330 Free PMC article.
-
Deep learning-based platform performs high detection sensitivity of intracranial aneurysms in 3D brain TOF-MRA: An external clinical validation study.Int J Med Inform. 2024 Aug;188:105487. doi: 10.1016/j.ijmedinf.2024.105487. Epub 2024 May 16. Int J Med Inform. 2024. PMID: 38761459
-
Comparison of Ultra-High-Resolution and Normal-Resolution CT-Angiography for Intracranial Aneurysm Detection in Patients with Subarachnoid Hemorrhage.Acad Radiol. 2024 Apr;31(4):1594-1604. doi: 10.1016/j.acra.2023.08.035. Epub 2023 Oct 9. Acad Radiol. 2024. PMID: 37821348
-
Diagnostic value of artificial intelligence-assisted CTA for the assessment of atherosclerosis plaque: a systematic review and meta-analysis.Front Cardiovasc Med. 2024 Sep 3;11:1398963. doi: 10.3389/fcvm.2024.1398963. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39290212 Free PMC article.
Cited by
-
Inconsistency of AI in intracranial aneurysm detection with varying dose and image reconstruction.Sci Rep. 2025 Jun 6;15(1):19921. doi: 10.1038/s41598-025-04830-7. Sci Rep. 2025. PMID: 40481138 Free PMC article.
-
Assessment of the stability of intracranial aneurysms using a deep learning model based on computed tomography angiography.Radiol Med. 2025 Feb;130(2):248-257. doi: 10.1007/s11547-024-01939-z. Epub 2024 Dec 12. Radiol Med. 2025. PMID: 39666223 Free PMC article.
-
Development of an indicator framework for assessing nursing quality in interventional therapy for intracranial aneurysms in China.Front Neurol. 2024 Dec 5;15:1403637. doi: 10.3389/fneur.2024.1403637. eCollection 2024. Front Neurol. 2024. PMID: 39703355 Free PMC article.
-
Methodological Challenges in Deep Learning-Based Detection of Intracranial Aneurysms: A Scoping Review.Neurointervention. 2025 Jul;20(2):52-65. doi: 10.5469/neuroint.2025.00283. Epub 2025 May 26. Neurointervention. 2025. PMID: 40415390 Free PMC article. Review.
-
Vessel-aware aneurysm detection using multi-scale deformable 3D attention.Med Image Comput Comput Assist Interv. 2024 Oct;15005:754-765. doi: 10.1007/978-3-031-72086-4_71. Epub 2024 Oct 4. Med Image Comput Comput Assist Interv. 2024. PMID: 40226842 Free PMC article.
References
-
- Etminan N., Chang H.S., Hackenberg K., De Rooij N.K., Vergouwen M.D., Rinkel G.J., Algra A. Worldwide incidence of aneurysmal subarachnoid hemorrhage according to region, time period, blood pressure, and smoking prevalence in the population: A systematic review and meta-analysis. JAMA Neurol. 2019;76:588–597. doi: 10.1001/jamaneurol.2019.0006. - DOI - PMC - PubMed
-
- Hoh B.L., Ko N.U., Amin-Hanjani S., Chou S.H.Y., Cruz-Flores S., Dangayach N.S., Derdeyn C.P., Du R., Hänggi D., Hetts S.W., et al. 2023 Guideline for the management of patients with aneurysmal subarachnoid hemorrhage: A guideline from the American Heart Association/American Stroke Association. Stroke. 2023;54:e314–e370. doi: 10.1161/STR.0000000000000436. - DOI - PubMed
-
- Siyanaki M.R.H., Lucke-Wold B., Khan M. Exploration of treatments for subarachnoid hemorrhage. J. Biomed Res. 2022;3:48 - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
