

Multifaceted Tissue-Protective Functions of Polyvalent Immunoglobulin Preparations in Severe Infections-Interactions with Neutrophils, Complement, and Coagulation Pathways
- PMID: 38002022
- PMCID: PMC10669904
- DOI: 10.3390/biomedicines11113022
Multifaceted Tissue-Protective Functions of Polyvalent Immunoglobulin Preparations in Severe Infections-Interactions with Neutrophils, Complement, and Coagulation Pathways
Abstract
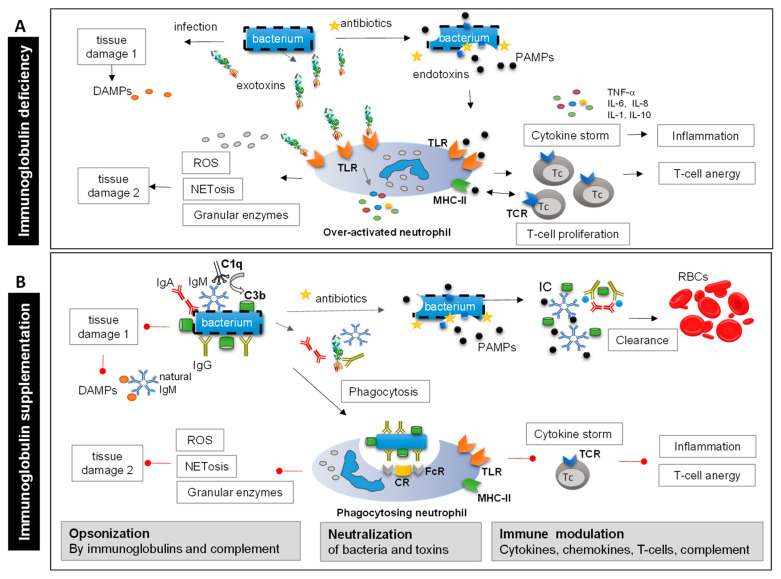
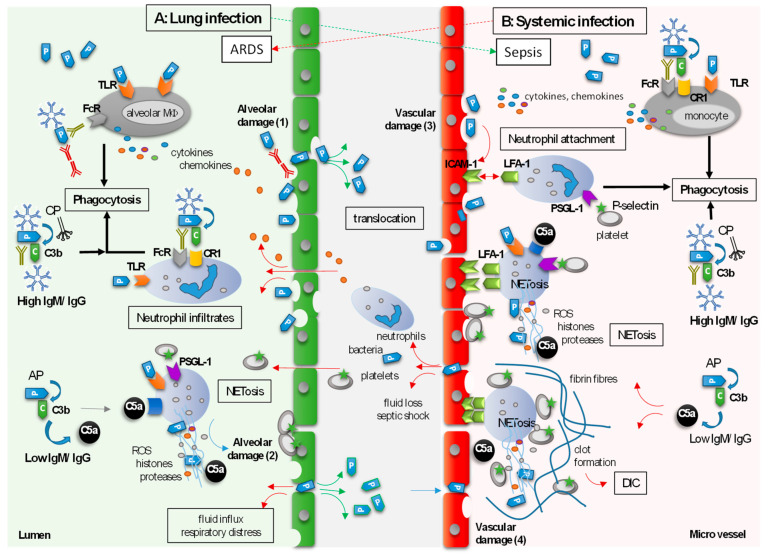
Severe infections induce immune defense mechanisms and initial tissue damage, which produce an inflammatory neutrophil response. Upon dysregulation of these responses, inflammation, further tissue damage, and systemic spread of the pathogen may occur. Subsequent vascular inflammation and activation of coagulation processes may cause microvascular obstruction at sites distal to the primary site of infection. Low immunoglobulin (Ig) M and IgG levels have been detected in patients with severe infections like sCAP and sepsis, associated with increased severity and mortality. Based on Ig's modes of action, supplementation with polyvalent intravenous Ig preparations (standard IVIg or IgM/IgA-enriched Ig preparations) has long been discussed as a treatment option for severe infections. A prerequisite seems to be the timely administration of Ig preparations before excessive tissue damage has occurred and coagulopathy has developed. This review focuses on nonclinical and clinical studies that evaluated tissue-protective activities resulting from interactions of Igs with neutrophils, complement, and the coagulation system. The data indicate that coagulopathy, organ failure, and even death of patients can possibly be prevented by the timely combined interactions of (natural) IgM, IgA, and IgG with neutrophils and complement.
Keywords: bacterial infection; coagulation; human polyvalent immunoglobulins; neutrophils; sCAP; sepsis; tissue damage.
Conflict of interest statement
The authors are full-time employees at Biotest, Dreieich, Germany, developing, manufacturing, and marketing plasma proteins and biotherapeutic drugs including IVIg (Intratect), Pentaglobin, and trimodulin.
Figures
Similar articles
-
Immunoglobulin M-enriched human intravenous immunoglobulins reduce leukocyte-endothelial cell interactions and attenuate microvascular perfusion failure in normotensive endotoxemia.Shock. 2008 Jan;29(1):133-9. doi: 10.1097/shk.0b013e318123e5a6. Shock. 2008. PMID: 18246604
-
The Dual Role of a Polyvalent IgM/IgA-Enriched Immunoglobulin Preparation in Activating and Inhibiting the Complement System.Biomedicines. 2021 Jul 14;9(7):817. doi: 10.3390/biomedicines9070817. Biomedicines. 2021. PMID: 34356880 Free PMC article.
-
The Functional Role of IgA in the IgM/IgA-Enriched Immunoglobulin Preparation Trimodulin.Biomedicines. 2021 Dec 3;9(12):1828. doi: 10.3390/biomedicines9121828. Biomedicines. 2021. PMID: 34944644 Free PMC article.
-
Limited Innovations After More Than 65 Years of Immunoglobulin Replacement Therapy: Potential of IgA- and IgM-Enriched Formulations to Prevent Bacterial Respiratory Tract Infections.Front Immunol. 2018 Aug 23;9:1925. doi: 10.3389/fimmu.2018.01925. eCollection 2018. Front Immunol. 2018. PMID: 30190722 Free PMC article. Review.
-
Janus face of complement-driven neutrophil activation during sepsis.Semin Immunol. 2018 Jun;37:12-20. doi: 10.1016/j.smim.2018.02.004. Epub 2018 Feb 14. Semin Immunol. 2018. PMID: 29454576 Review.
Cited by
-
Efficacy and safety of trimodulin in patients with severe COVID-19: results from a randomised, placebo-controlled, double-blind, multicentre, phase II trial (ESsCOVID).Eur J Med Res. 2024 Aug 13;29(1):418. doi: 10.1186/s40001-024-02008-x. Eur J Med Res. 2024. PMID: 39138518 Free PMC article. Clinical Trial.
-
The dysfunction of complement and coagulation in diseases: the implications for the therapeutic interventions.MedComm (2020). 2024 Oct 23;5(11):e785. doi: 10.1002/mco2.785. eCollection 2024 Nov. MedComm (2020). 2024. PMID: 39445002 Free PMC article. Review.
-
Prenatal Inflammation Reprograms Hypothalamic-Pituitary-Gonadal Axis Development in Female Rats.Inflammation. 2025 Feb 5. doi: 10.1007/s10753-025-02243-2. Online ahead of print. Inflammation. 2025. PMID: 39909991
-
Treatment with intravenous immunoglobulin modulates coagulation- and complement-related pathways in COVID-19 patients.Front Immunol. 2025 Jul 31;16:1623309. doi: 10.3389/fimmu.2025.1623309. eCollection 2025. Front Immunol. 2025. PMID: 40821834 Free PMC article.
References
-
- Evans L., Rhodes A., Alhazzani W., Antonelli M., Coopersmith C.M., French C., MacHado F.R., McIntyre L., Ostermann M., Prescott H.C., et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021;49:E1063–E1143. doi: 10.1097/CCM.0000000000005337. - DOI - PubMed
-
- Martin-Loeches I., Torres A., Nagavci B., Aliberti S., Antonelli M., Bassetti M., Bos L.D., Chalmers J.D., Derde L., de Waele J., et al. ERS/ESICM/ESCMID/ALAT guidelines for the management of severe community-acquired pneumonia. Intensive Care Med. 2023;49:615–632. doi: 10.1007/s00134-023-07033-8. - DOI - PMC - PubMed
-
- Metlay J.P., Waterer G.W., Long A.C., Anzueto A., Brozek J., Crothers K., Cooley L.A., Dean N.C., Fine M.J., Flanders S.A., et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019;200:e45–e67. doi: 10.1164/rccm.201908-1581ST. - DOI - PMC - PubMed
-
- Geier C., Schroder J., Tamm A., Dietz S., Nuding S., Holder K., Khandanpour O., Werdan K., Ebelt H. Influence of the serum levels of immunoglobulins on clinical outcomes in medical intensive-care patients. Med. Klin. Intensivmed. Notfmed. 2017;112:30–37. doi: 10.1007/s00063-015-0121-0. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
