

Why Intracranial Compliance Is Not Utilized as a Common Practical Tool in Clinical Practice
- PMID: 38002083
- PMCID: PMC10669292
- DOI: 10.3390/biomedicines11113083
Why Intracranial Compliance Is Not Utilized as a Common Practical Tool in Clinical Practice
Abstract
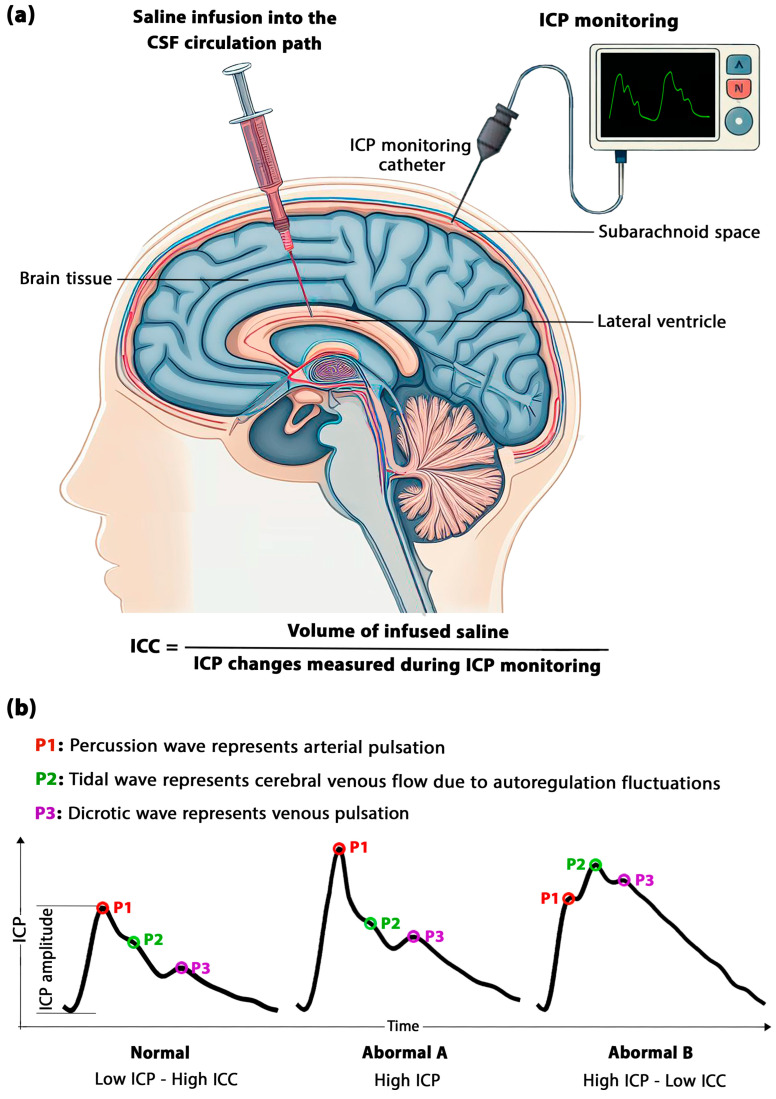
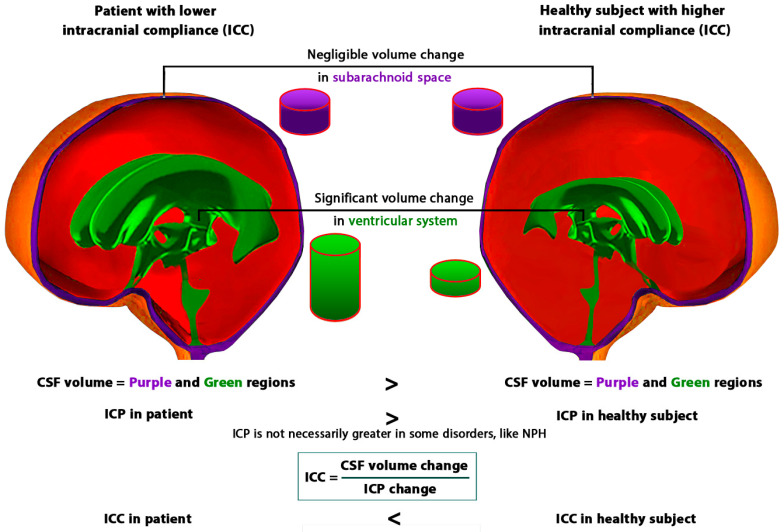
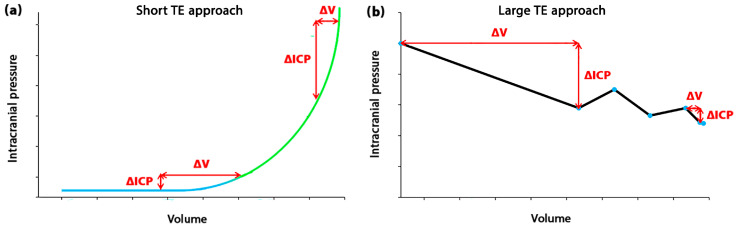
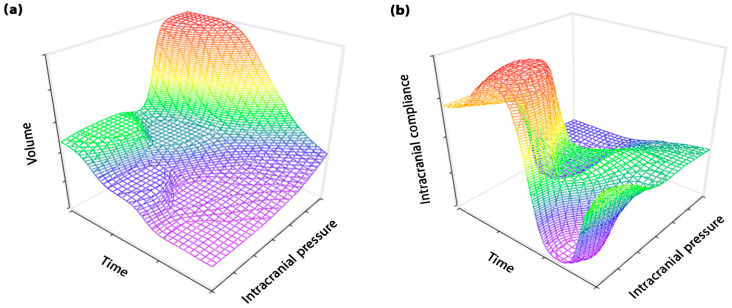
Intracranial compliance (ICC) holds significant potential in neuromonitoring, serving as a diagnostic tool and contributing to the evaluation of treatment outcomes. Despite its comprehensive concept, which allows consideration of changes in both volume and intracranial pressure (ICP), ICC monitoring has not yet established itself as a standard component of medical care, unlike ICP monitoring. This review highlighted that the first challenge is the assessment of ICC values, because of the invasive nature of direct measurement, the time-consuming aspect of non-invasive calculation through computer simulations, and the inability to quantify ICC values in estimation methods. Addressing these challenges is crucial, and the development of a rapid, non-invasive computer simulation method could alleviate obstacles in quantifying ICC. Additionally, this review indicated the second challenge in the clinical application of ICC, which involves the dynamic and time-dependent nature of ICC. This was considered by introducing the concept of time elapsed (TE) in measuring the changes in volume or ICP in the ICC equation (volume change/ICP change). The choice of TE, whether short or long, directly influences the ICC values that must be considered in the clinical application of the ICC. Compensatory responses of the brain exhibit non-monotonic and variable changes in long TE assessments for certain disorders, contrasting with the mono-exponential pattern observed in short TE assessments. Furthermore, the recovery behavior of the brain undergoes changes during the treatment process of various brain disorders when exposed to short and long TE conditions. The review also highlighted differences in ICC values across brain disorders with various strain rates and loading durations on the brain, further emphasizing the dynamic nature of ICC for clinical application. The insight provided in this review may prove valuable to professionals in neurocritical care, neurology, and neurosurgery for standardizing ICC monitoring in practical application related to the diagnosis and evaluation of treatment outcomes in brain disorders.
Keywords: brain biomechanics; brain disorder; cerebrospinal fluid; clinical application; diagnostic tool; gradual onset brain disorders; intracranial compliance (ICC); intracranial pressure (ICP); neurosurgery; viscous component.
Conflict of interest statement
The author declares no conflict of interest.
Figures
Similar articles
-
Feasibility of assessing non-invasive intracranial compliance using FSI simulation-based and MR elastography-based brain stiffness.Sci Rep. 2024 Mar 18;14(1):6493. doi: 10.1038/s41598-024-57250-4. Sci Rep. 2024. PMID: 38499758 Free PMC article.
-
Intracranial Compliance Concepts and Assessment: A Scoping Review.Front Neurol. 2021 Oct 25;12:756112. doi: 10.3389/fneur.2021.756112. eCollection 2021. Front Neurol. 2021. PMID: 34759884 Free PMC article.
-
A New Definition for Intracranial Compliance to Evaluate Adult Hydrocephalus After Shunting.Front Bioeng Biotechnol. 2022 Aug 1;10:900644. doi: 10.3389/fbioe.2022.900644. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 35979170 Free PMC article.
-
Analysis of magnetic resonance imaging-based blood and cerebrospinal fluid flow measurements in patients with Chiari I malformation: a system approach.Neurosurg Focus. 2001 Jul 15;11(1):E6. doi: 10.3171/foc.2001.11.1.7. Neurosurg Focus. 2001. PMID: 16724816 Clinical Trial.
-
Noninvasive intracranial compliance and pressure based on dynamic magnetic resonance imaging of blood flow and cerebrospinal fluid flow: review of principles, implementation, and other noninvasive approaches.Neurosurg Focus. 2003 Apr 15;14(4):e4. doi: 10.3171/foc.2003.14.4.4. Neurosurg Focus. 2003. PMID: 15679303 Review.
Cited by
-
Feasibility of assessing non-invasive intracranial compliance using FSI simulation-based and MR elastography-based brain stiffness.Sci Rep. 2024 Mar 18;14(1):6493. doi: 10.1038/s41598-024-57250-4. Sci Rep. 2024. PMID: 38499758 Free PMC article.
-
Serum Beta-Secretase 1 Activity Is a Potential Marker for the Differential Diagnosis between Alzheimer's Disease and Frontotemporal Dementia: A Pilot Study.Int J Mol Sci. 2024 Jul 30;25(15):8354. doi: 10.3390/ijms25158354. Int J Mol Sci. 2024. PMID: 39125924 Free PMC article.
-
Can magnetic resonance elastography serve as a diagnostic tool for gradual-onset brain disorders?Neurosurg Rev. 2023 Dec 7;47(1):3. doi: 10.1007/s10143-023-02238-3. Neurosurg Rev. 2023. PMID: 38062313 No abstract available.
-
Clinical Performance of the Brain4care System for Noninvasive Detection of Intracranial Hypertension.Neurocrit Care. 2025 Apr 28. doi: 10.1007/s12028-025-02273-6. Online ahead of print. Neurocrit Care. 2025. PMID: 40293697
-
Optimization of number and range of shunt valve performance levels in infant hydrocephalus: a machine learning analysis.Front Bioeng Biotechnol. 2024 Mar 18;12:1352490. doi: 10.3389/fbioe.2024.1352490. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 38562668 Free PMC article.
References
-
- Borlongan C.V., Burns J., Tajiri N., Stahl C.E., Weinbren N.L., Shojo H., Sanberg P.R., Emerich D.F., Kaneko Y., van Loveren H.R. Epidemiological survey-based formulae to approximate incidence and prevalence of neurological disorders in the United States: A meta-analysis. PLoS ONE. 2013;8:e78490. doi: 10.1371/journal.pone.0078490. - DOI - PMC - PubMed
-
- Reeves B.C., Karimy J.K., Kundishora A.J., Mestre H., Cerci H.M., Matouk C., Alper S.L., Lundgaard I., Nedergaard M., Kahle K.T. Glymphatic system impairment in Alzheimer’s disease and idiopathic normal pressure hydrocephalus. Trends Mol. Med. 2020;26:285–295. doi: 10.1016/j.molmed.2019.11.008. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
