

Functional Magnetic Resonance Imaging and Diffusion Tensor Imaging-Tractography in Resective Brain Surgery: Lesion Coverage Strategies and Patient Outcomes
- PMID: 38002534
- PMCID: PMC10670090
- DOI: 10.3390/brainsci13111574
Functional Magnetic Resonance Imaging and Diffusion Tensor Imaging-Tractography in Resective Brain Surgery: Lesion Coverage Strategies and Patient Outcomes
Abstract
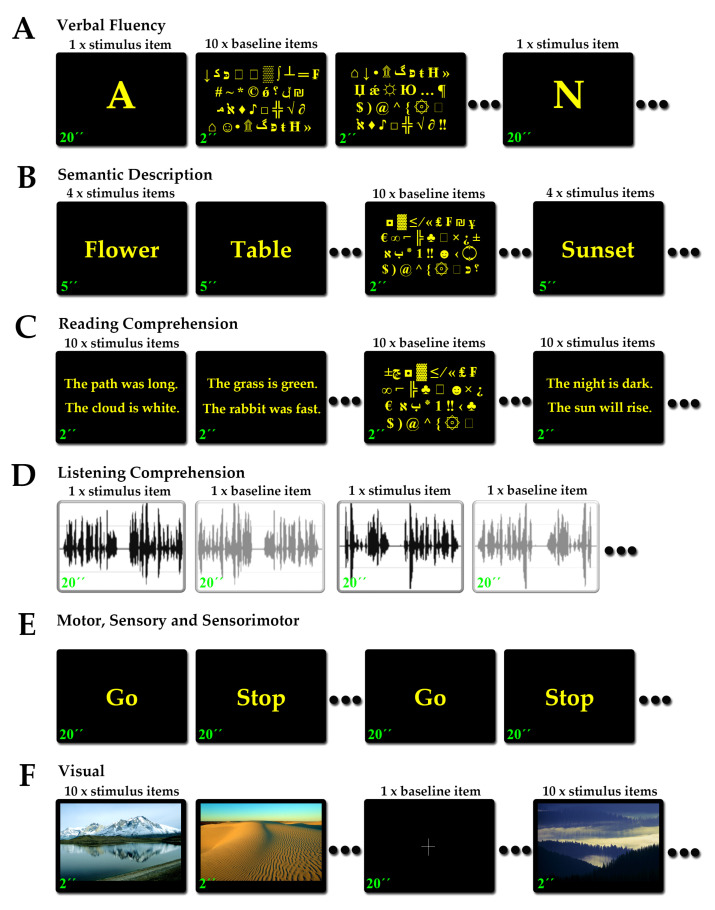
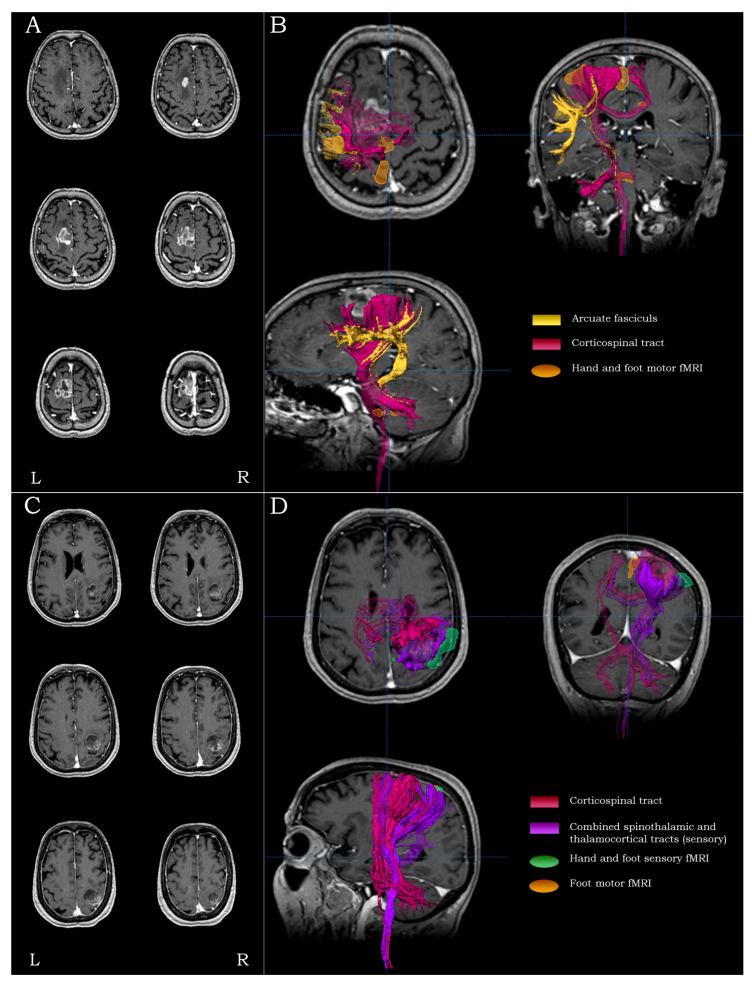
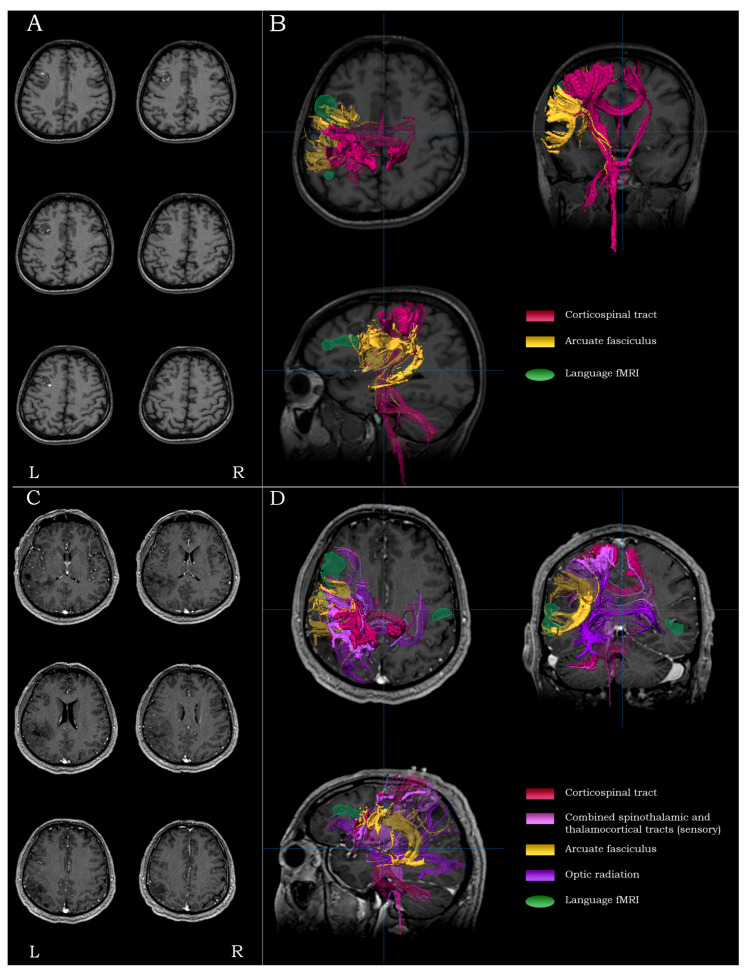
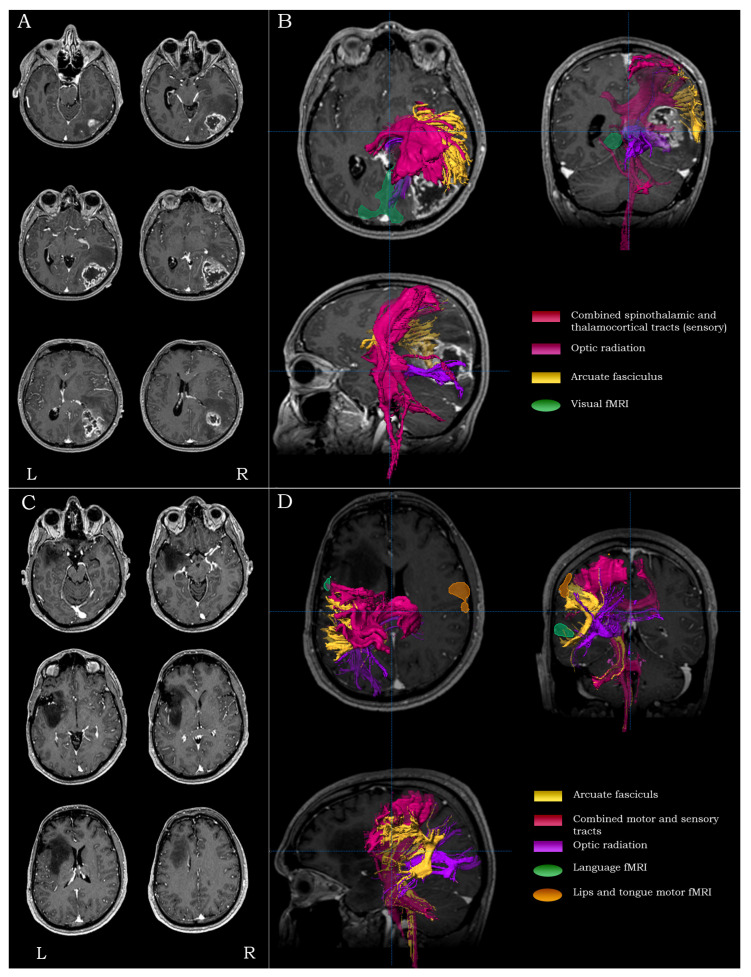
Diffusion tensor imaging (DTI)-tractography and functional magnetic resonance imaging (fMRI) have dynamically entered the presurgical evaluation context of brain surgery during the past decades, providing novel perspectives in surgical planning and lesion access approaches. However, their application in the presurgical setting requires significant time and effort and increased costs, thereby raising questions regarding efficiency and best use. In this work, we set out to evaluate DTI-tractography and combined fMRI/DTI-tractography during intra-operative neuronavigation in resective brain surgery using lesion-related preoperative neurological deficit (PND) outcomes as metrics. We retrospectively reviewed medical records of 252 consecutive patients admitted for brain surgery. Standard anatomical neuroimaging protocols were performed in 127 patients, 69 patients had additional DTI-tractography, and 56 had combined DTI-tractography/fMRI. fMRI procedures involved language, motor, somatic sensory, sensorimotor and visual mapping. DTI-tractography involved fiber tracking of the motor, sensory, language and visual pathways. At 1 month postoperatively, DTI-tractography patients were more likely to present either improvement or preservation of PNDs (p = 0.004 and p = 0.007, respectively). At 6 months, combined DTI-tractography/fMRI patients were more likely to experience complete PND resolution (p < 0.001). Low-grade lesion patients (N = 102) with combined DTI-tractography/fMRI were more likely to experience complete resolution of PNDs at 1 and 6 months (p = 0.001 and p < 0.001, respectively). High-grade lesion patients (N = 140) with combined DTI-tractography/fMRI were more likely to have PNDs resolved at 6 months (p = 0.005). Patients with motor symptoms (N = 80) were more likely to experience complete remission of PNDs at 6 months with DTI-tractography or combined DTI-tractography/fMRI (p = 0.008 and p = 0.004, respectively), without significant difference between the two imaging protocols (p = 1). Patients with sensory symptoms (N = 44) were more likely to experience complete PND remission at 6 months with combined DTI-tractography/fMRI (p = 0.004). The intraoperative neuroimaging modality did not have a significant effect in patients with preoperative seizures (N = 47). Lack of PND worsening was observed at 6 month follow-up in patients with combined DTI-tractography/fMRI. Our results strongly support the combined use of DTI-tractography and fMRI in patients undergoing resective brain surgery for improving their postoperative clinical profile.
Keywords: DTI-tractography; brain tumor surgery; fMRI; neuronavigation; presurgical evaluation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Functional Magnetic Resonance Imaging (fMRI), Pre-intraoperative Tractography in Neurosurgery: The Experience of Sant' Andrea Rome University Hospital.Acta Neurochir Suppl. 2017;124:241-250. doi: 10.1007/978-3-319-39546-3_36. Acta Neurochir Suppl. 2017. PMID: 28120080
-
Associations between clinical outcome and navigated transcranial magnetic stimulation characteristics in patients with motor-eloquent brain lesions: a combined navigated transcranial magnetic stimulation-diffusion tensor imaging fiber tracking approach.J Neurosurg. 2018 Mar;128(3):800-810. doi: 10.3171/2016.11.JNS162322. Epub 2017 Mar 31. J Neurosurg. 2018. PMID: 28362239
-
Functional neuronavigation combined with intra-operative 3D ultrasound: initial experiences during surgical resections close to eloquent brain areas and future directions in automatic brain shift compensation of preoperative data.Acta Neurochir (Wien). 2007;149(4):365-78. doi: 10.1007/s00701-006-1110-0. Epub 2007 Feb 19. Acta Neurochir (Wien). 2007. PMID: 17308976
-
Tractography and the connectome in neurosurgical treatment of gliomas: the premise, the progress, and the potential.Neurosurg Focus. 2020 Feb 1;48(2):E6. doi: 10.3171/2019.11.FOCUS19785. Neurosurg Focus. 2020. PMID: 32006950 Free PMC article. Review.
-
Preoperative surgical planning of glioma: limitations and reliability of fMRI and DTI tractography.J Neurosurg Sci. 2019 Apr;63(2):127-134. doi: 10.23736/S0390-5616.18.04597-6. Epub 2018 Oct 2. J Neurosurg Sci. 2019. PMID: 30290696 Review.
Cited by
-
Addressing neurological complications of emerging infectious diseases: a neurosurgical perspective.Neurosurg Rev. 2024 Sep 19;47(1):635. doi: 10.1007/s10143-024-02841-y. Neurosurg Rev. 2024. Retraction in: Neurosurg Rev. 2025 Feb 4;48(1):167. doi: 10.1007/s10143-025-03322-6. PMID: 39294399 Retracted. No abstract available.
-
Modernizing Neuro-Oncology: The Impact of Imaging, Liquid Biopsies, and AI on Diagnosis and Treatment.Int J Mol Sci. 2025 Jan 22;26(3):917. doi: 10.3390/ijms26030917. Int J Mol Sci. 2025. PMID: 39940686 Free PMC article. Review.
-
AI-Driven innovations for managing ependymoma in neurosurgery.Neurosurg Rev. 2024 Sep 11;47(1):590. doi: 10.1007/s10143-024-02871-6. Neurosurg Rev. 2024. Retraction in: Neurosurg Rev. 2025 Feb 8;48(1):219. doi: 10.1007/s10143-025-03368-6. PMID: 39256263 Retracted. No abstract available.
References
-
- Afra D., Osztie E., Sipos L., Vitanovics D. Preoperative history and postoperative survival of supratentorial low-grade astrocytomas. Br. J. Neurosurg. 1999;13:299–305. - PubMed
-
- Aghi M.K., Nahed B.V., Sloan A.E., Ryken T.C., Kalkanis S.N., Olson J.J. The role of surgery in the management of patients with diffuse low grade glioma: A systematic review and evidence-based clinical practice guideline. J. Neurooncol. 2015;125:503–530. doi: 10.1007/s11060-015-1867-1. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
