

New-Onset Atrial Fibrillation in the Critically Ill COVID-19 Patients Hospitalized in the Intensive Care Unit
- PMID: 38002603
- PMCID: PMC10672690
- DOI: 10.3390/jcm12226989
New-Onset Atrial Fibrillation in the Critically Ill COVID-19 Patients Hospitalized in the Intensive Care Unit
Abstract
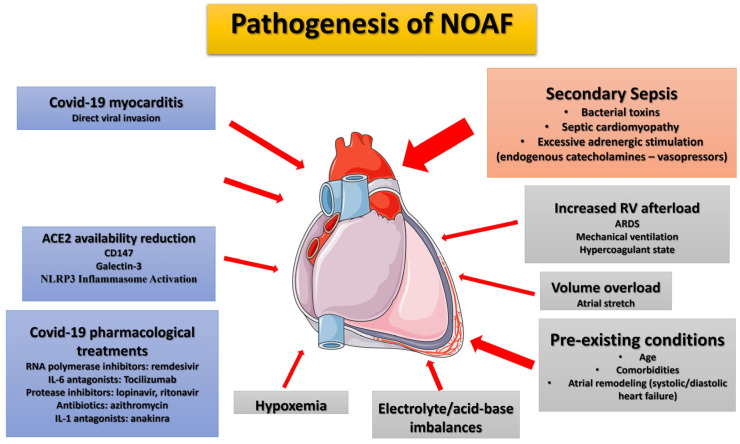
New-onset atrial fibrillation (NOAF) is the most frequently encountered cardiac arrhythmia observed in patients with COVID-19 infection, particularly in Intensive Care Unit (ICU) patients. The purpose of the present review is to delve into the occurrence of NOAF in COVID-19 and thoroughly review recent, pertinent data. However, the causality behind this connection has yet to be thoroughly explored. The proposed mechanisms that could contribute to the development of AF in these patients include myocardial damage resulting from direct virus-induced cardiac injury, potentially leading to perimyocarditis; a cytokine crisis and heightened inflammatory response; hypoxemia due to acute respiratory distress; disturbances in acid-base and electrolyte levels; as well as the frequent use of adrenergic drugs in critically ill patients. Additionally, secondary bacterial sepsis and septic shock have been suggested as primary causes of NOAF in ICU patients. This notion gains strength from the observation of a similar prevalence of NOAF in septic non-COVID ICU patients with ARDS. It is plausible that both myocardial involvement from SARS-CoV-2 and secondary sepsis play pivotal roles in the onset of arrhythmia in ICU patients. Nonetheless, there exists a significant variation in the prevalence of NOAF among studies focused on severe COVID-19 cases with ARDS. This discrepancy could be attributed to the inclusion of mixed populations with varying degrees of illness severity, encompassing not only patients in general wards but also those admitted to the ICU, whether intubated or not. Furthermore, the occurrence of NOAF is linked to increased morbidity and mortality. However, it remains to be determined whether NOAF independently influences outcomes in critically ill COVID-19 ICU patients or if it merely reflects the disease's severity. Lastly, the management of NOAF in these patients has not been extensively studied. Nevertheless, the current guidelines for NOAF in non-COVID ICU patients appear to be effective, while accounting for the specific drugs used in COVID-19 treatment that may prolong the QT interval (although drugs like lopinavir/ritonavir, hydrochlorothiazide, and azithromycin have been discontinued) or induce bradycardia (e.g., remdesivir).
Keywords: COVID-19; ICU; critical illness; new-onset atrial fibrillation; trigger factors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Complications of new-onset atrial fibrillation in critically ill COVID-19 patients admitted to the intensive care unit (ICU): a meta-analysis.BMC Cardiovasc Disord. 2024 Aug 5;24(1):407. doi: 10.1186/s12872-024-04086-5. BMC Cardiovasc Disord. 2024. PMID: 39103764 Free PMC article.
-
Secondary bacterial infections are a leading factor triggering New Onset Atrial Fibrillation in intubated ICU Covid-19 ARDS patients.J Infect Public Health. 2022 Jul;15(7):766-772. doi: 10.1016/j.jiph.2022.06.006. Epub 2022 Jun 16. J Infect Public Health. 2022. PMID: 35724437 Free PMC article.
-
Prevalence, Risk Factors, and Mortality of New-Onset Atrial Fibrillation in Mechanically Ventilated Critically Ill Patients.J Clin Med. 2024 Nov 9;13(22):6750. doi: 10.3390/jcm13226750. J Clin Med. 2024. PMID: 39597893 Free PMC article.
-
CHA2DS2-VASc Score as Predictor of New-Onset Atrial Fibrillation and Mortality in Critical COVID-19 Patients.J Intensive Care Med. 2024 Nov;39(11):1155-1163. doi: 10.1177/08850666241272068. Epub 2024 Aug 7. J Intensive Care Med. 2024. PMID: 39109625 Review.
-
Beyond the Beat: A Multifaceted Review of Atrial Fibrillation in Sepsis: Risk Factors, Management Strategies, and Economic Impact.Cardiol Res. 2025 Feb;16(1):1-14. doi: 10.14740/cr1723. Epub 2024 Dec 31. Cardiol Res. 2025. PMID: 39897439 Free PMC article. Review.
Cited by
-
Association between triglyceride-glucose index and mortality in critically ill patients with atrial fibrillation: a retrospective cohort study.Cardiovasc Diabetol. 2025 Mar 24;24(1):138. doi: 10.1186/s12933-025-02697-6. Cardiovasc Diabetol. 2025. PMID: 40128768 Free PMC article.
-
Complications of new-onset atrial fibrillation in critically ill COVID-19 patients admitted to the intensive care unit (ICU): a meta-analysis.BMC Cardiovasc Disord. 2024 Aug 5;24(1):407. doi: 10.1186/s12872-024-04086-5. BMC Cardiovasc Disord. 2024. PMID: 39103764 Free PMC article.
References
-
- Phua J., Weng L., Ling L., Egi M., Lim C.M., Divatia J.V., Shrestha B.R., Arabi Y.M., Ng J., Gomersall C.D., et al. Intensive care management of coronavirus disease 2019 (COVID-19): Challenges and recommendations. Lancet Respir. Med. 2020;8:506–517. doi: 10.1016/S2213-2600(20)30161-2. - DOI - PMC - PubMed
-
- Grasselli G., Zangrillo A., Zanella A., Antonelli M., Cabrini L., Castelli A., Cereda D., Coluccello A., Foti G., Fumagalli R., et al. COVID-19 Lombardy ICU Network. Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323:1574–1581. doi: 10.1001/jama.2020.5394. - DOI - PMC - PubMed
-
- Cummings M.J., Baldwin M.R., Abrams D., Jacobson S.D., Meyer B.J., Balough E.M., Aaron J.G., Claassen J., Rabbani L.E., Hastie J., et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet. 2020;395:1763–1770. doi: 10.1016/S0140-6736(20)31189-2. - DOI - PMC - PubMed
-
- Wang Y., Shu H., Liu H., Li X., Zhou X., Zou X., Pan S., Xu J., Xu D., Zhao X., et al. The peak levels of highly sensitive troponin I predicts in-hospital mortality in COVID-19 patients with cardiac injury: A retrospective study. Eur. Heart J. Acute Cardiovasc. Care. 2021;10:6–15. doi: 10.1093/ehjacc/zuaa019. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
