

Femoral Occlusion during Neonatal Cardiopulmonary Resuscitation Improves Outcomes in an Ovine Model of Perinatal Cardiac Arrest
- PMID: 38002895
- PMCID: PMC10670492
- DOI: 10.3390/children10111804
Femoral Occlusion during Neonatal Cardiopulmonary Resuscitation Improves Outcomes in an Ovine Model of Perinatal Cardiac Arrest
Abstract
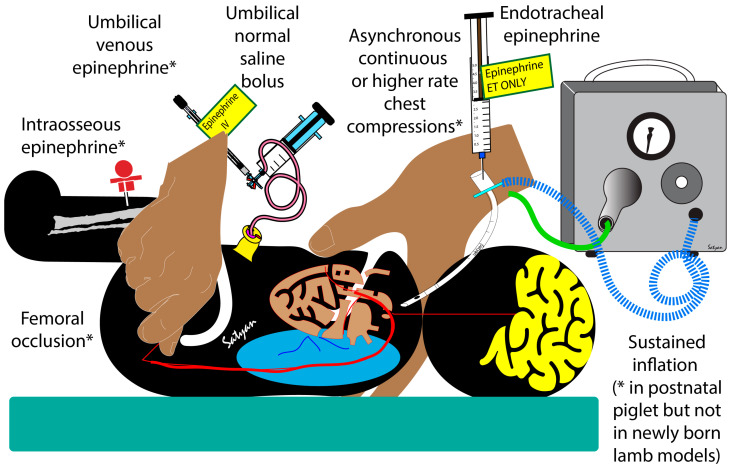
Background: The goal of chest compressions during neonatal resuscitation is to increase cerebral and coronary blood flow leading to the return of spontaneous circulation (ROSC). During chest compressions, bilateral femoral occlusion may increase afterload and promote carotid and coronary flow, an effect similar to epinephrine. Our objectives were to determine the impact of bilateral femoral occlusion during chest compressions on the incidence and timing of ROSC and hemodynamics.
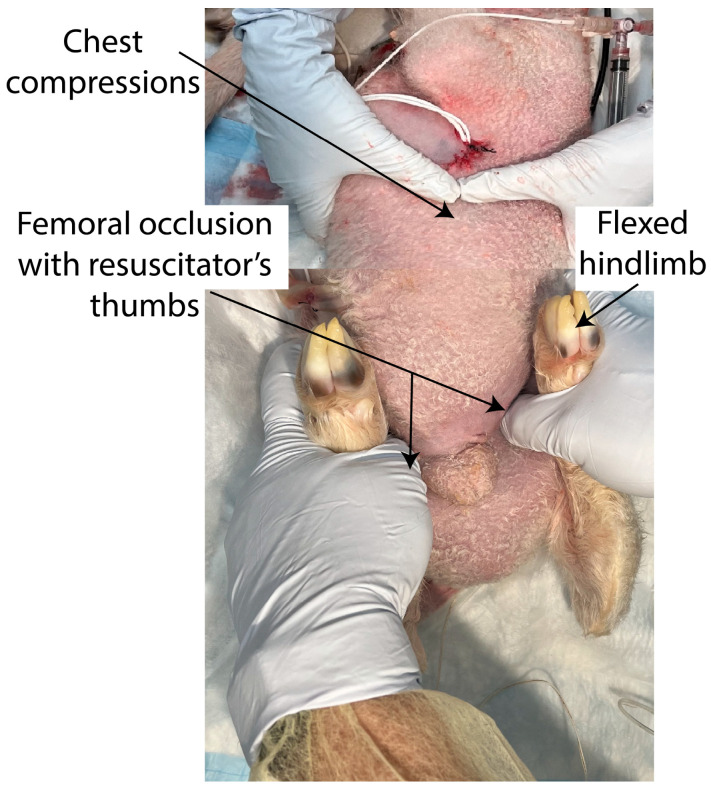
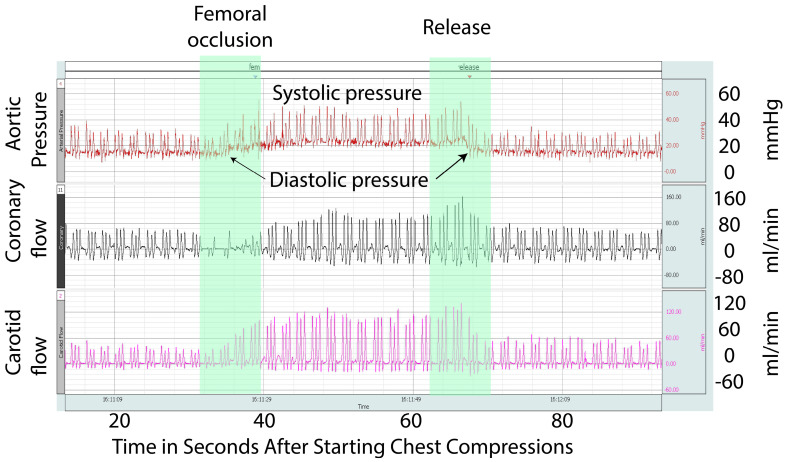
Methodology: In this randomized study, 19 term fetal lambs in cardiac arrest were resuscitated based on the Neonatal Resuscitation Program guidelines and randomized into two groups: femoral occlusion or controls. Bilateral femoral arteries were occluded by applying pressure using two fingers during chest compressions.
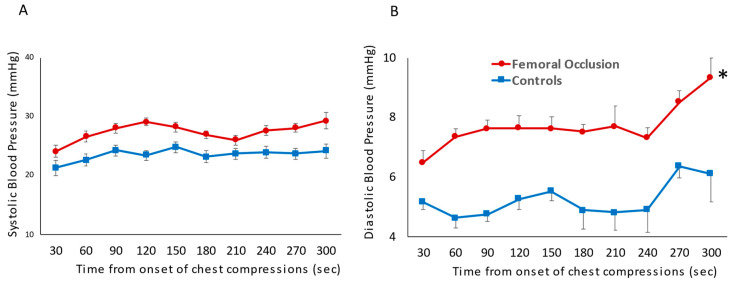
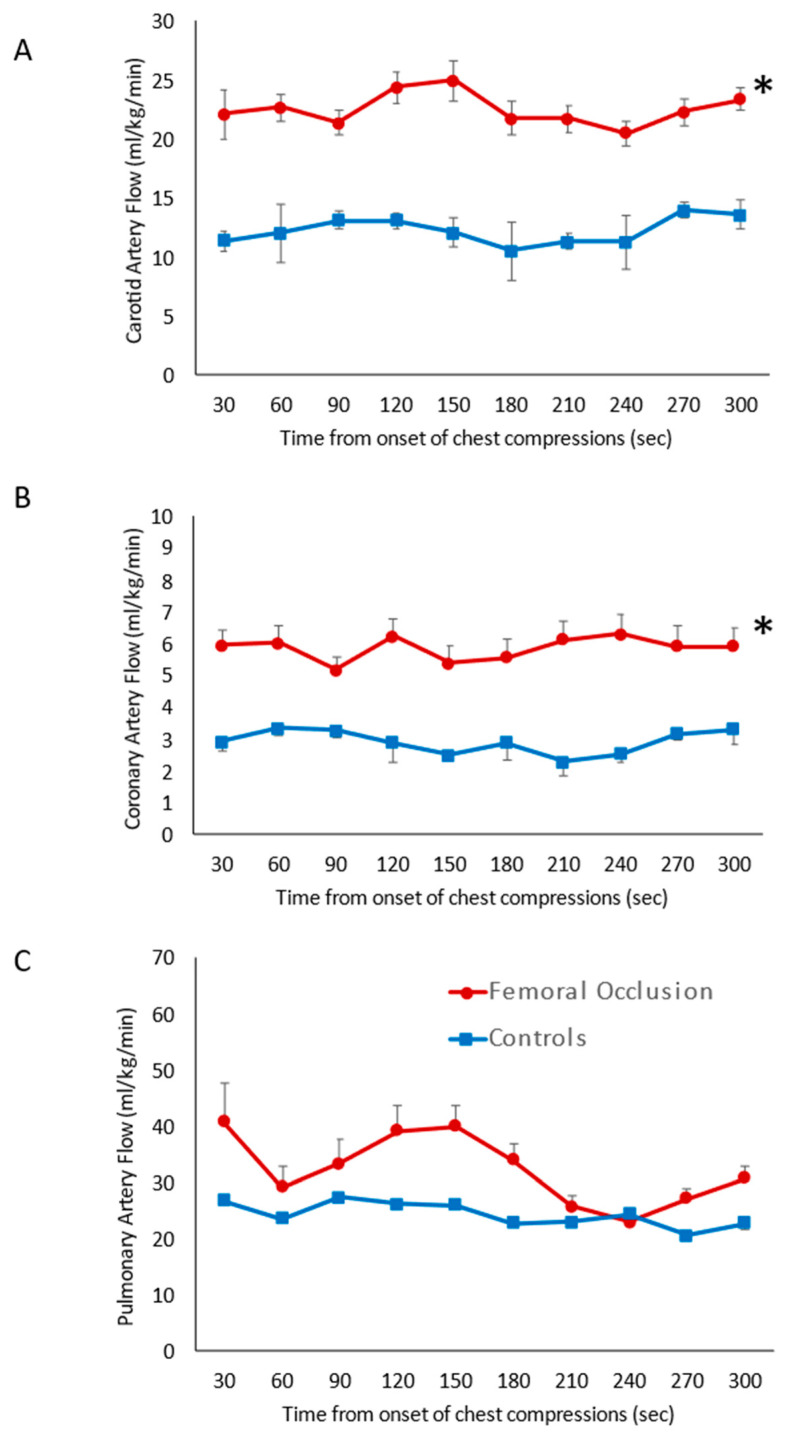
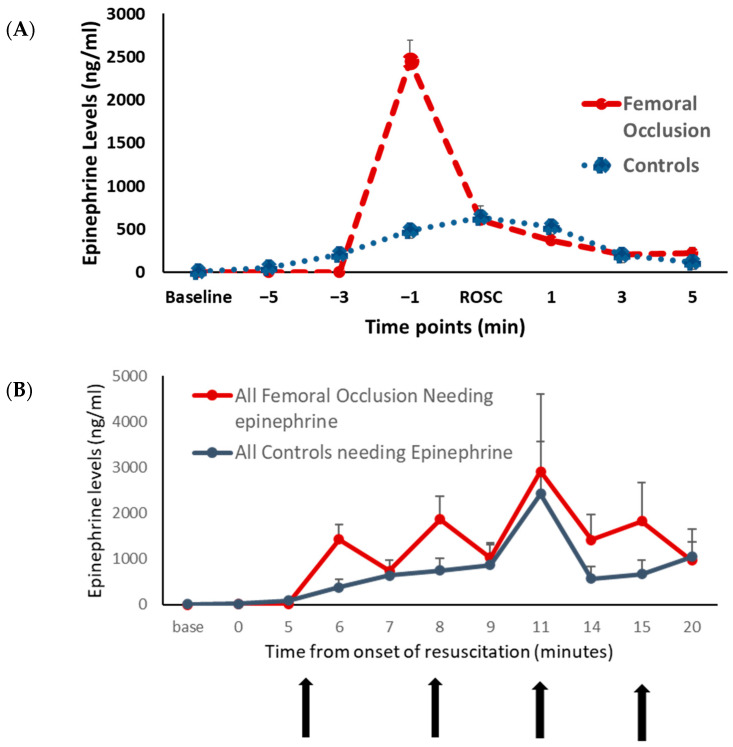
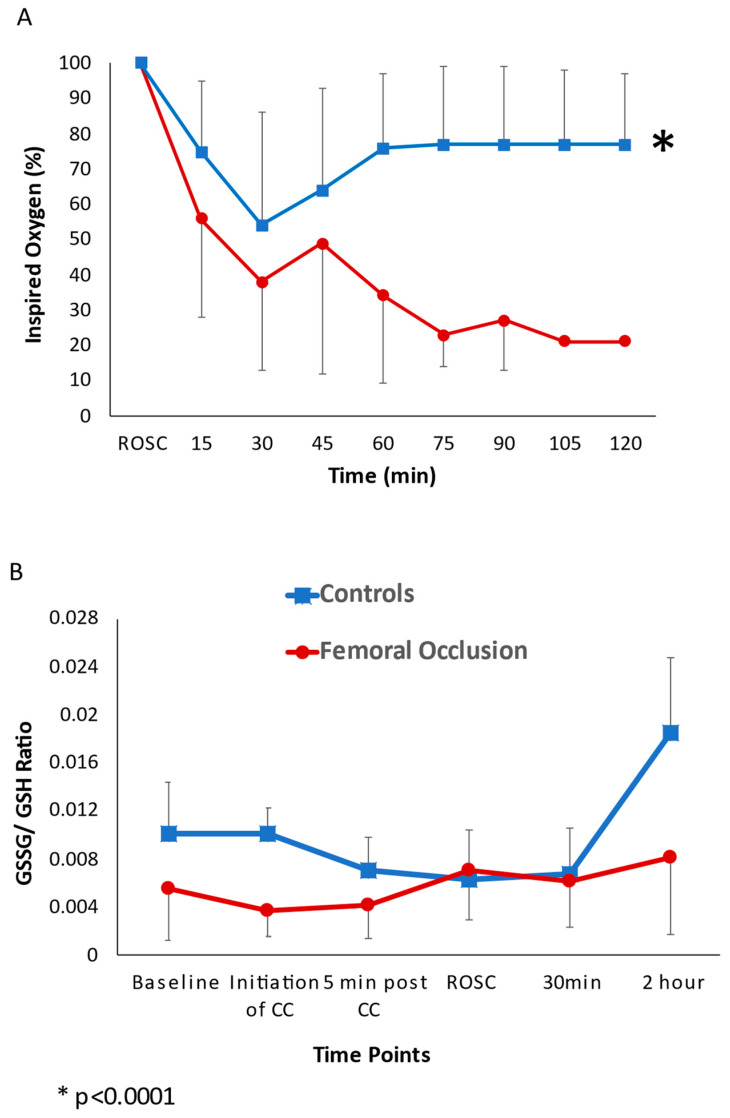
Results: Seventy percent (7/10) of the lambs in the femoral occlusion group achieved ROSC in 5 ± 2 min and three lambs (30%) did not receive epinephrine. ROSC was achieved in 44% (4/9) of the controls in 13 ± 6 min and all lambs received epinephrine. The femoral occlusion group had higher diastolic blood pressures, carotid and coronary blood flow.
Conclusion: Femoral occlusion resulted in faster and higher incidence of ROSC, most likely due to attaining increased diastolic pressures, coronary and carotid flow. This is a low-tech intervention that can be easily adapted in resource limited settings, with the potential to improve survival and neurodevelopmental outcomes.
Keywords: chest compression; femoral occlusion; neonatal resuscitation.
Conflict of interest statement
The authors declare no conflict of interest. Dr. Satyan Lakshminrusimha was a member of the AAP-NRP steering committee during this study period. The views expressed in this presentation are those of the authors and do not represent the official position of AAP or NRP.
Figures
References
-
- Wyckoff M.H., Salhab W.A., Heyne R.J., Kendrick D.E., Stoll B.J., Laptook A.R., National Institute of Child Health and Human Development Neonatal Research Network Outcome of extremely low birth weight infants who received delivery room cardiopulmonary resuscitation. J. Pediatr. 2012;160:239–244.e2. doi: 10.1016/j.jpeds.2011.07.041. - DOI - PMC - PubMed
-
- Hayakawa K., Tasaki O., Hamasaki T., Sakai T., Shiozaki T., Nakagawa Y., Ogura H., Kuwagata Y., Kajino K., Iwami T., et al. Prognostic indicators and outcome prediction model for patients with return of spontaneous circulation from cardiopulmonary arrest: The Utstein Osaka Project. Resuscitation. 2011;82:874–880. doi: 10.1016/j.resuscitation.2011.02.045. - DOI - PubMed
-
- Vali P., Chandrasekharan P., Rawat M., Gugino S., Koenigsknecht C., Helman J., Mathew B., Berkelhamer S., Nair J., Wyckoff M., et al. Hemodynamics and gas exchange during chest compressions in neonatal resuscitation. PLoS ONE. 2017;12:e0176478. doi: 10.1371/journal.pone.0176478. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
