

The Value of ER∝ in the Prognosis of GH- and PRL-Secreting PitNETs: Clinicopathological Correlations
- PMID: 38003353
- PMCID: PMC10671753
- DOI: 10.3390/ijms242216162
The Value of ER∝ in the Prognosis of GH- and PRL-Secreting PitNETs: Clinicopathological Correlations
Abstract
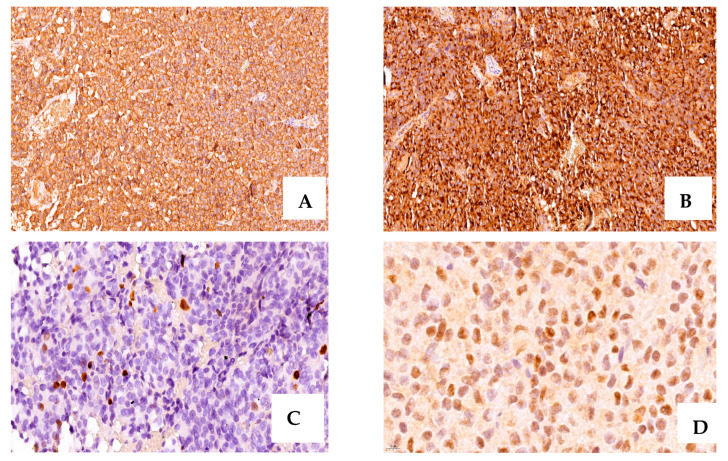
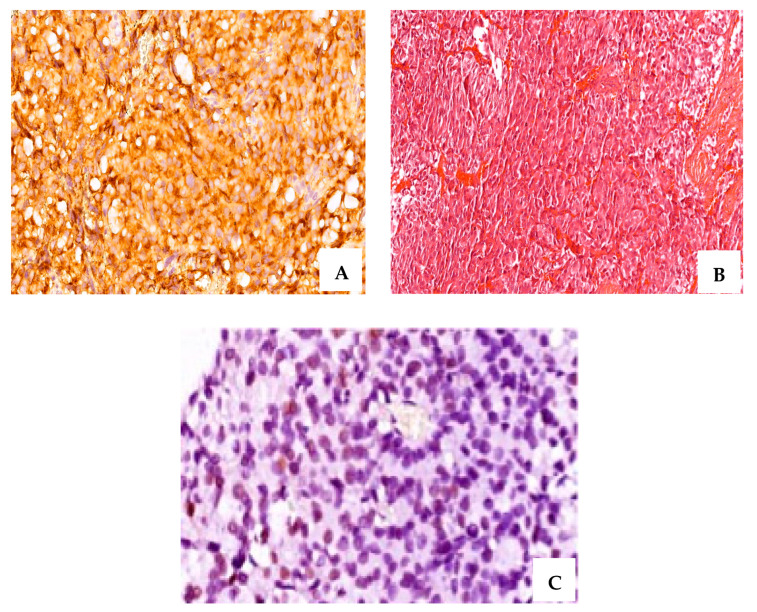
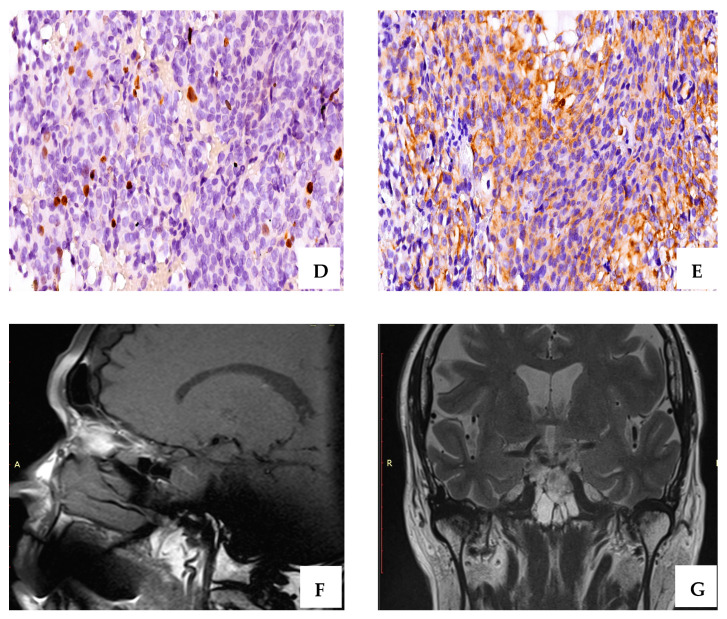
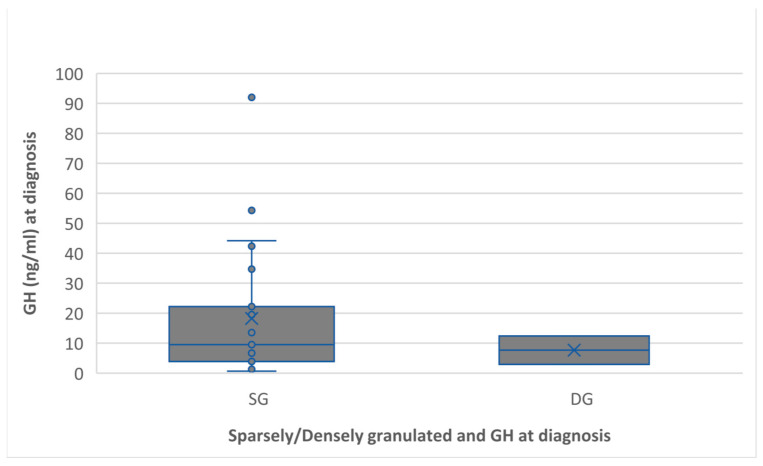
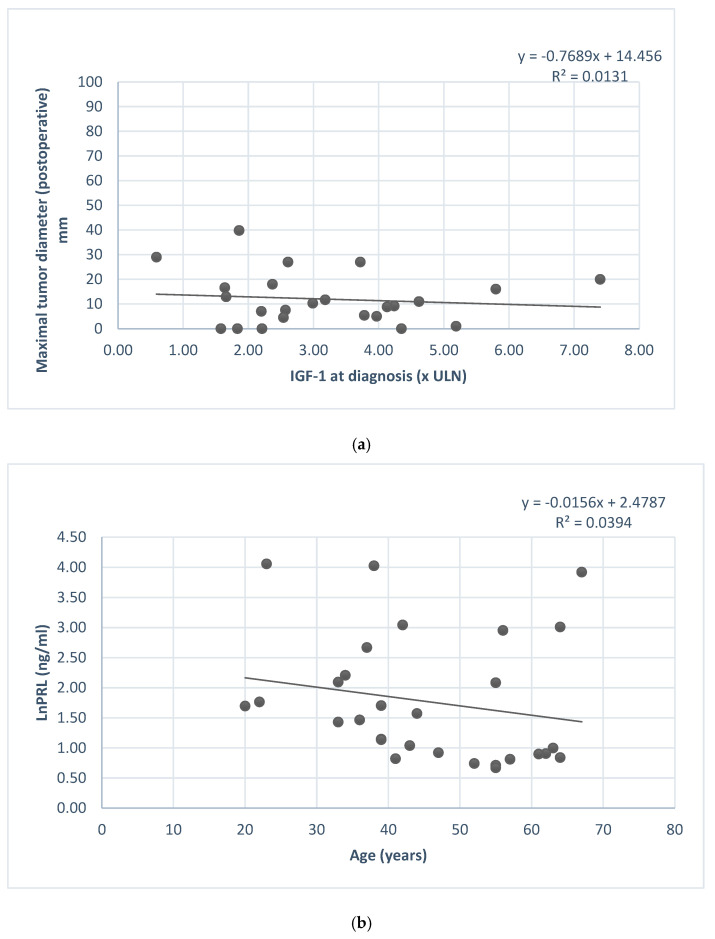
Pituitary neuroendocrine tumors (PitNETs) are divided into multiple histological subtypes, which determine their clinical and biological variable behavior. Despite their benign evolution, in some cases, prolactin (PRL) and growth hormone (GH)-secreting PitNETs may have aggressive behavior. In this study, we investigated the potential predictive role of ER∝, alongside the clinicopathological classification of PitNETs (tumor diameter, tumor type, and tumor grade). A retrospective study was conducted with 32 consecutive cases of PRL- and mixed GH- and PRL-secreting PitNETs (5 patients with prolactinomas and 27 with acromegaly, among them, 7 patients with GH- and PRL- co-secretion) who underwent transsphenoidal intervention. Tumor specimens were histologically and immunohistochemical examined: anterior pituitary hormones, ki-67 labeling index, CAM 5.2, and ER∝; ER∝ expression was correlated with basal PRL levels at diagnosis (rho = 0.60, p < 0.01) and postoperative PRL levels (rho = 0.58, p < 0.001). In our study, the ER∝ intensity score was lower in female patients. Postoperative maximal tumor diameter correlated with Knosp grade (p = 0.02); CAM 5.2 pattern (densely/sparsely granulated/mixed densely and sparsely granulated) was correlated with postoperative PRL level (p = 0.002), and with ki-67 (p < 0.001). The IGF1 level at diagnosis was correlated with the postoperative GH nadir value in the oral glucose tolerance test (OGTT) (rho = 0.52, p < 0.05). Also, basal PRL level at diagnosis was correlated with postoperative tumor diameter (p = 0.63, p < 0.001). At univariate logistic regression, GH nadir in OGTT test at diagnostic, IGF1, gender, and invasion were independent predictors of remission for mixed GH- and PRL-secreting Pit-NETs; ER∝ can be used as a prognostic marker and loss of ER∝ expression should be considered a sign of lower differentiation and a likely indicator of poor prognosis. A sex-related difference can be considered in the evolution and prognosis of these tumors, but further studies are needed to confirm this hypothesis.
Keywords: GH- and PRL-secreting PitNET; PRL-secreting PitNET; estrogen receptor alpha; pituitary neuroendocrine tumor; prognostic factors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Navigating prognostic strategies for GH- and PRL-secreting pituitary neuroendocrine tumors: key insights from a clinicopathological study.Front Endocrinol (Lausanne). 2025 Apr 10;16:1541514. doi: 10.3389/fendo.2025.1541514. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40276548 Free PMC article.
-
Novel features of tumors that secrete both growth hormone and prolactin in acromegaly.Neurosurgery. 1994 Aug;35(2):179-83; discussion 183-4. doi: 10.1227/00006123-199408000-00001. Neurosurgery. 1994. PMID: 7969823
-
Synchronous Multiple Pituitary Neuroendocrine Tumors of Different Cell Lineages.Endocr Pathol. 2018 Dec;29(4):332-338. doi: 10.1007/s12022-018-9545-4. Endocr Pathol. 2018. PMID: 30215160
-
GH-Secreting Adenoma or Tumor? Issues in Pituitary Neoplasms Nomenclature, Classification, and Characterization.Front Horm Res. 2024;55:119-132. doi: 10.1159/000539946. Front Horm Res. 2024. PMID: 39586264 Review.
-
Pleiomorphism plurihormonal Pit-1-positive macroadenoma with central hyperthyroidism: a rare case report and literature review.BMC Endocr Disord. 2022 Dec 21;22(1):325. doi: 10.1186/s12902-022-01220-2. BMC Endocr Disord. 2022. PMID: 36539773 Free PMC article. Review.
Cited by
-
Predictors of growth hormone level on postoperative day one in patients with acromegaly.Endocrine. 2025 Apr;88(1):249-261. doi: 10.1007/s12020-024-04130-6. Epub 2024 Dec 20. Endocrine. 2025. PMID: 39707075 Free PMC article.
-
Navigating prognostic strategies for GH- and PRL-secreting pituitary neuroendocrine tumors: key insights from a clinicopathological study.Front Endocrinol (Lausanne). 2025 Apr 10;16:1541514. doi: 10.3389/fendo.2025.1541514. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40276548 Free PMC article.
-
Predictors of therapeutic failure in GH and prolactin co-secreting pituitary adenomas.Endocr Connect. 2025 Jul 15;14(7):e250103. doi: 10.1530/EC-25-0103. Print 2025 Jul 1. Endocr Connect. 2025. PMID: 40590355 Free PMC article.
References
-
- Besser M. Criteria for medical as opposed to surgical treatment of prolactinomas. Acta Endocrinol. 1993;129:27–30. - PubMed
-
- Cozzi R., Auriemma R.S., De Menis E., Esposito F., Ferrante E., Iatì G., Mazzatenta D., Poggi M., Rudà R., Tortora F., et al. Italian Guidelines for the Management of Prolactinomas. Endocr. Metab. Immune Disord. Drug Targets. 2023;23:1459–1479. doi: 10.2174/1871530323666230511104045. - DOI - PMC - PubMed
-
- Jiang Y., Yin S., Hu Y., Chen C., Ma W., Jiang S., Zhou P. Mammosomatotroph and mixed somatotroph-lactotroph adenoma in acromegaly: A retrospective study with long-term follow-up. Endocrine. 2019;66:310–318. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
