

Endotoxic Septic Shock: Diagnosis and Treatment
- PMID: 38003374
- PMCID: PMC10671446
- DOI: 10.3390/ijms242216185
Endotoxic Septic Shock: Diagnosis and Treatment
Abstract
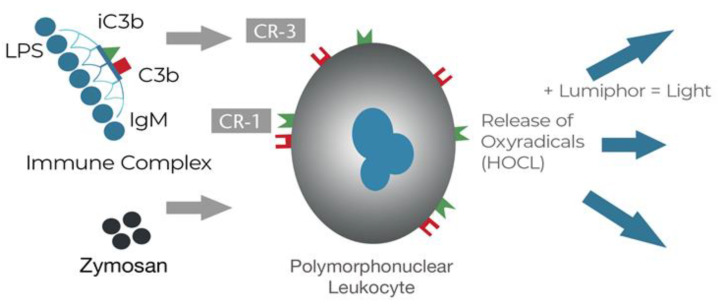
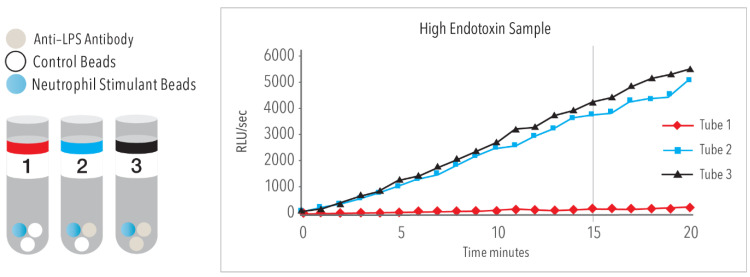
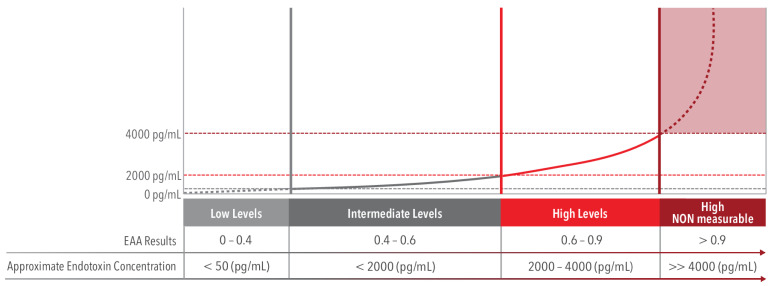
Endotoxin, also referred to as lipopolysaccharide (LPS), is a potent stimulator of the inflammatory cascade which may progress to sepsis and septic shock. The term endotoxic septic shock has been used for patients who have a clinical phenotype that is characterized by high endotoxin activity in addition to a high burden of organ failure; especially a pattern of organ failure including hepatic dysfunction, acute kidney injury, and various forms of endothelial dysfunction. Endotoxic septic shock has been a target for drug therapy for decades with no success. A likely barrier to their success was the inability to quantify endotoxin in the bloodstream. The Endotoxin Activity Assay (EAA) is positioned to change this landscape. In addition, medical devices using adsorptive technology in an extra-corporeal circulation has been shown to remove large quantities of endotoxin from the bloodstream. Focusing on the use of EAA to determine high concentrations of endotoxin will allow patients with endotoxic septic shock to be identified quickly and these patients may benefit most from removal of endotoxin using extracorporeal methods.
Keywords: diagnosis of endotoxemia; endotoxic septic shock; endotoxin; sepsis.
Conflict of interest statement
D. M. Foster is a consultant for and J.A. Kellum is an employee of Spectral Medical Inc., the manufacturer of the endotoxin activity assay (EAA). Spectral Medical is also the holder of the license of the PMX cartridge and sponsor of the Tigris clinical study.
Figures

Similar articles
-
The role of endotoxin in septic shock.Crit Care. 2023 Oct 19;27(1):400. doi: 10.1186/s13054-023-04690-5. Crit Care. 2023. PMID: 37858258 Free PMC article. Review.
-
Abdominal Septic Shock - Endotoxin Adsorption Treatment (ASSET) - endotoxin removal in abdominal and urogenital septic shock with the Alteco® LPS Adsorber: study protocol for a double-blinded, randomized placebo-controlled trial.Trials. 2016 Dec 8;17(1):587. doi: 10.1186/s13063-016-1723-4. Trials. 2016. PMID: 27931259 Free PMC article. Clinical Trial.
-
Therapeutic Rationale for Endotoxin Removal with Polymyxin B Immobilized Fiber Column (PMX) for Septic Shock.Int J Mol Sci. 2021 Feb 23;22(4):2228. doi: 10.3390/ijms22042228. Int J Mol Sci. 2021. PMID: 33672437 Free PMC article. Review.
-
The golden hour of polymyxin B hemoperfusion in endotoxic shock: The basis for sequential extracorporeal therapy in sepsis.Artif Organs. 2020 Feb;44(2):184-186. doi: 10.1111/aor.13550. Epub 2019 Sep 2. Artif Organs. 2020. PMID: 31386769 Free PMC article.
-
Treatment of sepsis by extracorporeal elimination of endotoxin using polymyxin B-immobilized fiber.Am J Surg. 1994 Apr;167(4):412-7. doi: 10.1016/0002-9610(94)90126-0. Am J Surg. 1994. PMID: 8179086
Cited by
-
Nonlinear relationship between Hemoglobin-to-Age Ratio and all-cause mortality in patients with septic shock: A retrospective cohort study in the MIMIC-IV database.PLoS One. 2024 Dec 6;19(12):e0313937. doi: 10.1371/journal.pone.0313937. eCollection 2024. PLoS One. 2024. PMID: 39642117 Free PMC article.
-
Monotropein inhibits MMP9-mediated cardiac oxidative stress, inflammation, matrix degradation and apoptosis in a mouse and cell line models of septic cardiac injury.Mol Biol Rep. 2025 Mar 20;52(1):329. doi: 10.1007/s11033-025-10421-6. Mol Biol Rep. 2025. PMID: 40111530
-
The Value of Serum Procalcitonin, Thromboelastography Combined with Platelet Count in Predicting the Short-Term Progression of Septic Shock in the Intensive Care Unit.Int J Gen Med. 2024 Jul 31;17:3361-3370. doi: 10.2147/IJGM.S464566. eCollection 2024. Int J Gen Med. 2024. PMID: 39100724 Free PMC article.
-
The value of NT-proBNP, NLR, Ang-1 combined with APACHE II and SOFA scores in evaluating 28-day mortality of septic shock.Medicine (Baltimore). 2025 Jun 6;104(23):e42547. doi: 10.1097/MD.0000000000042547. Medicine (Baltimore). 2025. PMID: 40489844 Free PMC article.
-
Research trends and hotspots on septic shock: a bibliometric study and visualization analysis.Front Med (Lausanne). 2024 Nov 27;11:1490462. doi: 10.3389/fmed.2024.1490462. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39664313 Free PMC article.
References
-
- Mouncey P.R., Osborn T.M., Power G.S., Harrison D.A., Sadique M.Z., Grieve R.D., Jahan R., Tan J.C., Harvey S., Bell D., et al. Protocolised Management in Sepsis (ProMISe): A multicentre randomised controlled trial of the clinical effectiveness and cost-effectiveness of early, goal-directed, protocolised resuscitation for emerging septic shock. Health Technol. Assess. 2015;19:i-150. doi: 10.3310/hta19970. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
