

Immune Status of Individuals with Traumatic Spinal Cord Injury: A Systematic Review and Meta-Analysis
- PMID: 38003575
- PMCID: PMC10670917
- DOI: 10.3390/ijms242216385
Immune Status of Individuals with Traumatic Spinal Cord Injury: A Systematic Review and Meta-Analysis
Abstract
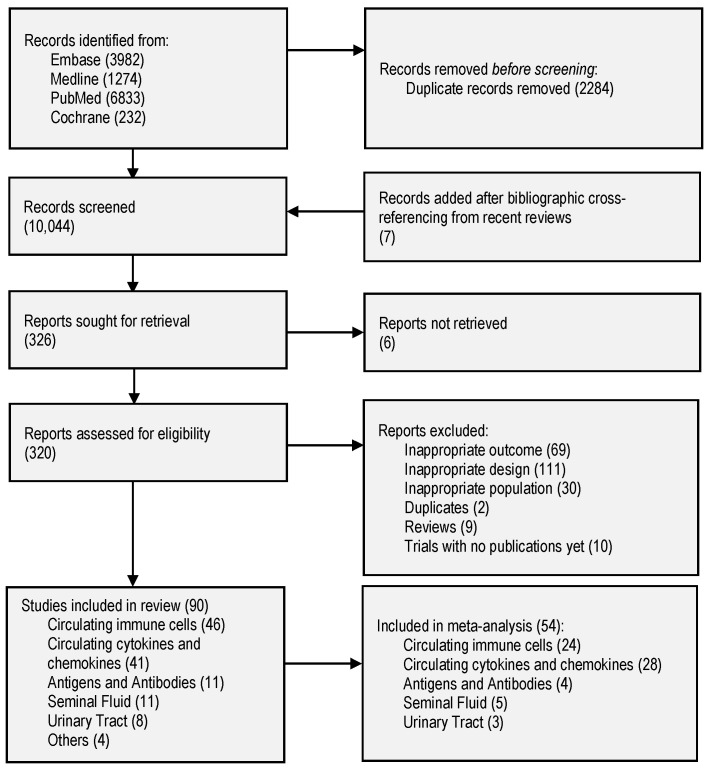
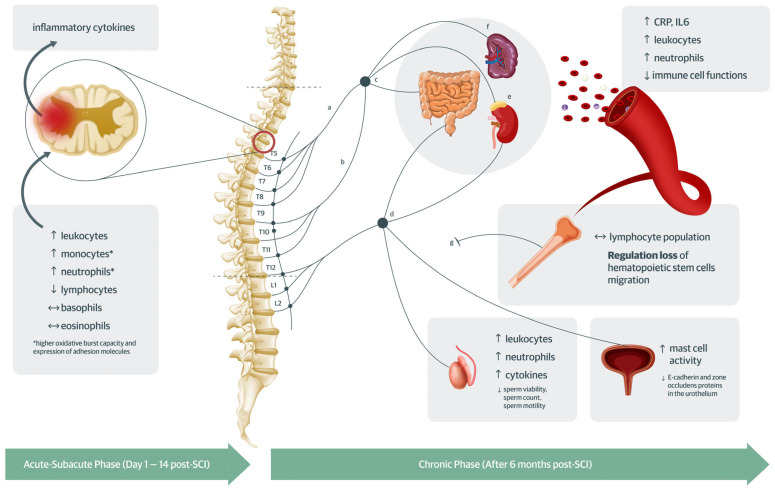
Individuals with spinal cord injury (SCI) have higher infection rates compared to those without SCI. In this review, the immune status difference between individuals with and without traumatic SCI is investigated by examining their peripheral immune cells and markers. PubMed, Cochrane, EMBASE, and Ovid MEDLINE were searched without language or date restrictions. Studies reporting peripheral immune markers' concentration and changes in functional capabilities of immune cells that compared individuals with and without SCI were included. Studies with participants with active infection, immune disease, and central nervous system (CNS) immune markers were excluded. The review followed the PRISMA guidelines. Effect estimates were measured by Weighted Mean Difference (WMD) using a random-effects model. Study quality was assessed using the National Heart, Lung, and Blood Institute Quality Assessment Tool. Fifty-four studies (1813 with SCI and 1378 without SCI) contributed to the meta-analysis. Leukocytes (n = 23, WMD 0.78, 95% CI 0.17; 1.38, I2 83%), neutrophils (n = 11, WMD 0.76, 95% CI 0.09; 1.42, I2 89%), C-reactive protein (CRP) (n = 12, WMD 2.25, 95% CI 1.14; 3.56, I2 95%), and IL6 (n = 13, WMD 2.33, 95% CI 1.20; 3.49, I2 97%) were higher in individuals with SCI vs. without SCI. Clinical factors (phase of injury, completeness of injury, sympathetic innervation impairment, age, sex) and study-related factors (sample size, study design, and serum vs. plasma) partially explained heterogeneity. Immune cells exhibited lower functional capability in individuals with SCI vs. those without SCI. Most studies (75.6%) had a moderate risk of bias. The immune status of individuals with SCI differs from those without SCI and is clinically influenced by the phase of injury, completeness of injury, sympathetic innervation impairment, age, and sex. These results provide information that is vital for monitoring and management strategies to effectively improve the immune status of individuals with SCI.
Keywords: immune depression; immunology; meta-analysis; traumatic spinal cord injury.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
Similar articles
-
Technological aids for the rehabilitation of memory and executive functioning in children and adolescents with acquired brain injury.Cochrane Database Syst Rev. 2016 Jul 1;7(7):CD011020. doi: 10.1002/14651858.CD011020.pub2. Cochrane Database Syst Rev. 2016. PMID: 27364851 Free PMC article.
-
Effectiveness and tolerability of pharmacologic and combined interventions for reducing injection pain during routine childhood immunizations: systematic review and meta-analyses.Clin Ther. 2009;31 Suppl 2:S104-51. doi: 10.1016/j.clinthera.2009.08.001. Clin Ther. 2009. PMID: 19781433
-
Electronic cigarettes for smoking cessation.Cochrane Database Syst Rev. 2022 Nov 17;11(11):CD010216. doi: 10.1002/14651858.CD010216.pub7. Cochrane Database Syst Rev. 2022. Update in: Cochrane Database Syst Rev. 2024 Jan 8;1:CD010216. doi: 10.1002/14651858.CD010216.pub8. PMID: 36384212 Free PMC article. Updated.
-
Negative pressure wound therapy for open traumatic wounds.Cochrane Database Syst Rev. 2018 Jul 3;7(7):CD012522. doi: 10.1002/14651858.CD012522.pub2. Cochrane Database Syst Rev. 2018. PMID: 29969521 Free PMC article.
-
Prognosis of adults and children following a first unprovoked seizure.Cochrane Database Syst Rev. 2023 Jan 23;1(1):CD013847. doi: 10.1002/14651858.CD013847.pub2. Cochrane Database Syst Rev. 2023. PMID: 36688481 Free PMC article.
Cited by
-
Plasma fibrinogen level is independent risk factor associated with the incidence of pulmonary infection in patients with spinal cord injury: a retrospective cohort study.BMC Pulm Med. 2024 Oct 18;24(1):520. doi: 10.1186/s12890-024-03332-y. BMC Pulm Med. 2024. PMID: 39425165 Free PMC article.
-
Multifaceted Pathophysiology and Secondary Complications of Chronic Spinal Cord Injury: Focus on Pressure Injury.J Clin Med. 2025 Feb 26;14(5):1556. doi: 10.3390/jcm14051556. J Clin Med. 2025. PMID: 40095463 Free PMC article. Review.
-
Characterization of the Expressions and m6A Methylation Modification Patterns of mRNAs and lncRNAs in a Spinal Cord Injury Rat Model.Mol Neurobiol. 2025 Jan;62(1):806-818. doi: 10.1007/s12035-024-04297-z. Epub 2024 Jun 22. Mol Neurobiol. 2025. PMID: 38907070 Free PMC article.
-
Immunoregulation of Glia after spinal cord injury: a bibliometric analysis.Front Immunol. 2024 Jun 13;15:1402349. doi: 10.3389/fimmu.2024.1402349. eCollection 2024. Front Immunol. 2024. PMID: 38938572 Free PMC article.
-
Effects of Uro-Vaxom vs. placebo on the urinary tract microbiome in individuals with spinal cord injury in a randomized controlled pilot trial (Uro-Vaxom pilot).Sci Rep. 2025 Apr 14;15(1):12825. doi: 10.1038/s41598-025-96939-y. Sci Rep. 2025. PMID: 40229352 Free PMC article. Clinical Trial.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
