

Anomalous Left Coronary Artery from the Pulmonary Artery: How to Diagnose and Treat
- PMID: 38003878
- PMCID: PMC10672344
- DOI: 10.3390/jpm13111561
Anomalous Left Coronary Artery from the Pulmonary Artery: How to Diagnose and Treat
Abstract
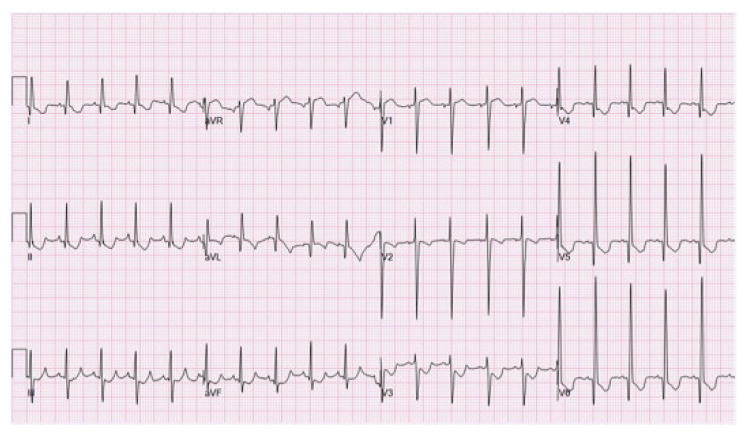
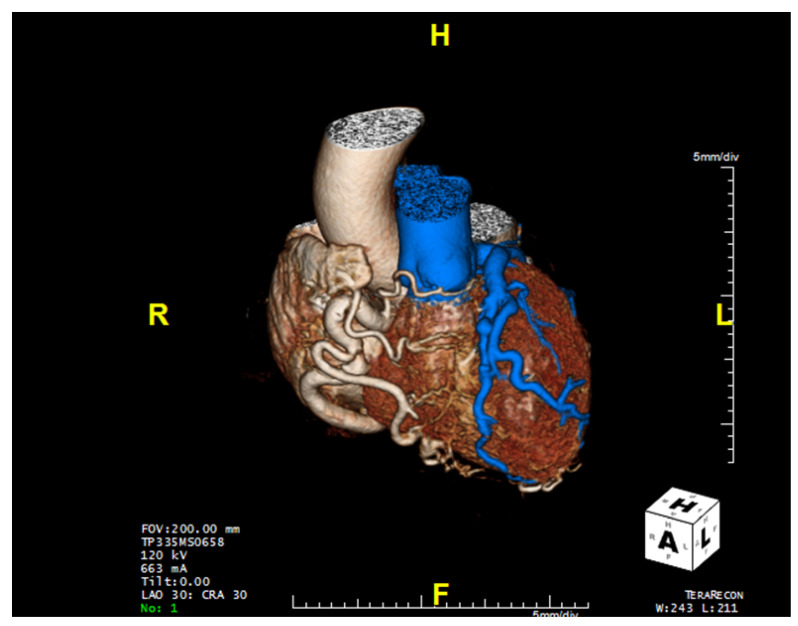
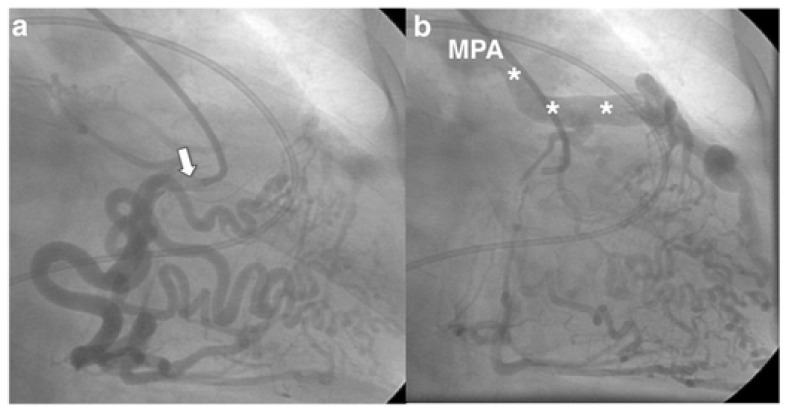
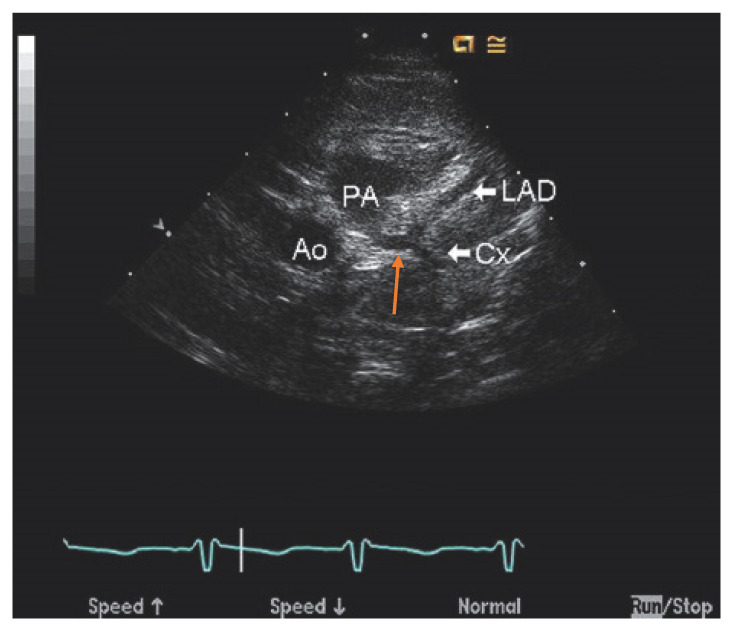
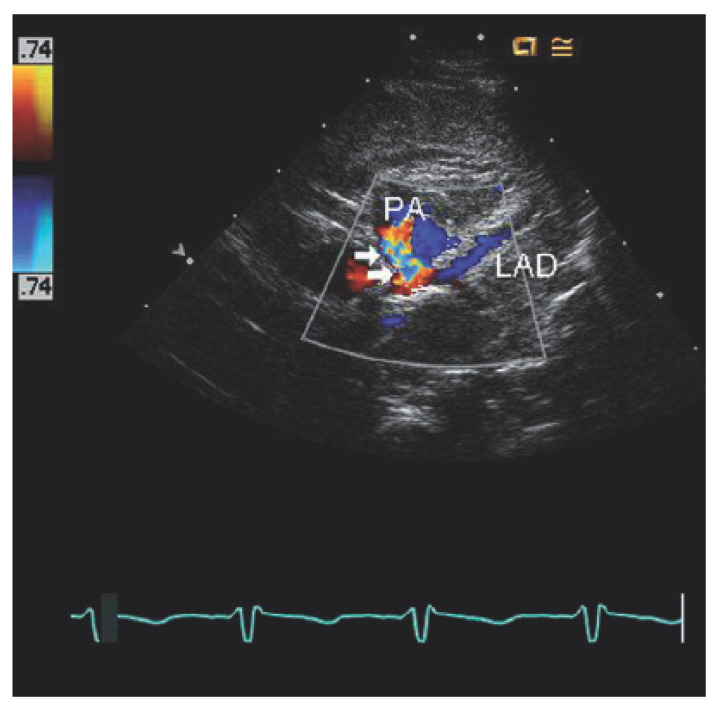
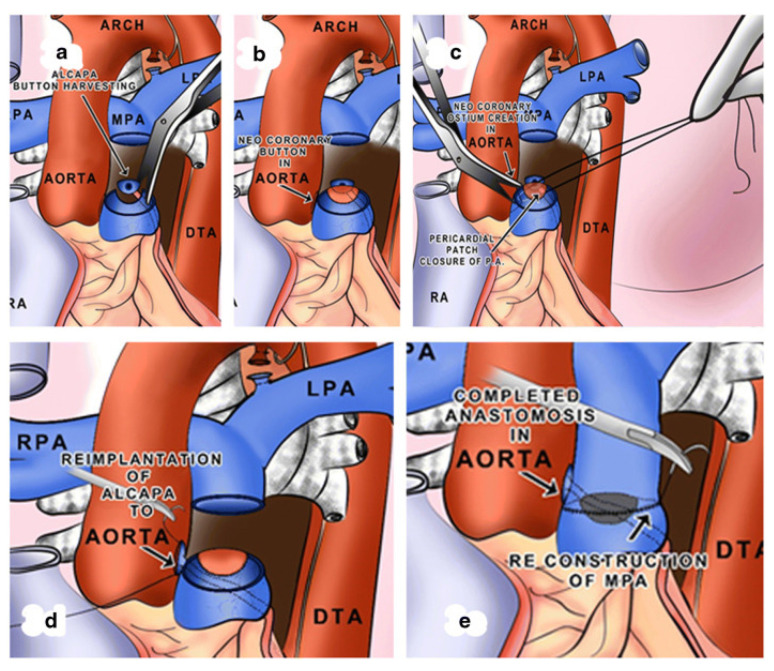
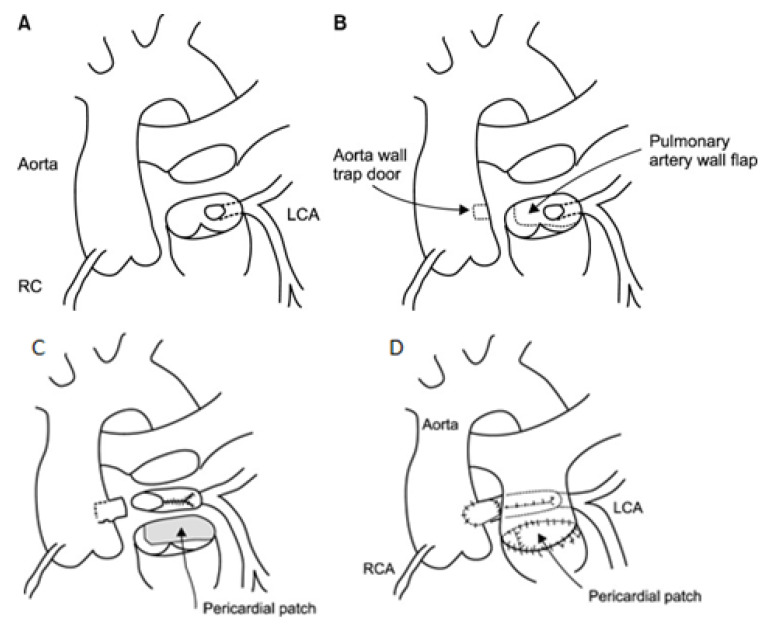
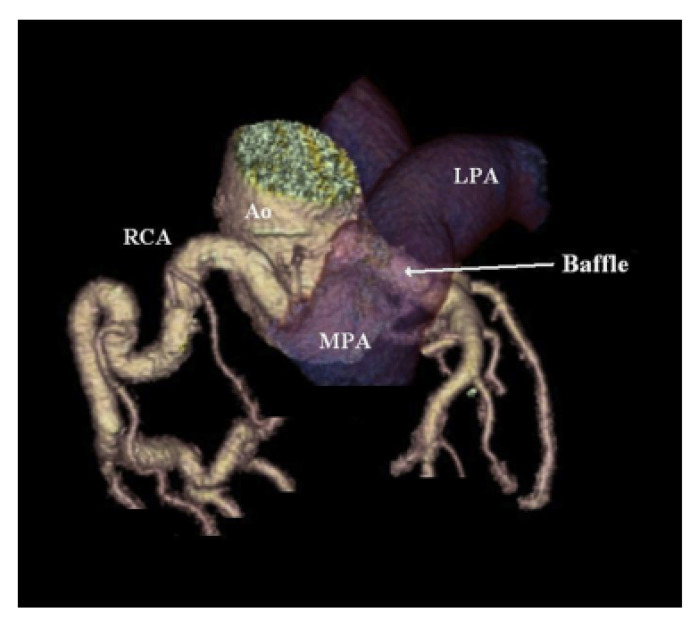
Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) is a rare coronary anomaly that can present in childhood or adulthood with a multitude of symptoms depending on the age of presentation. It should be suspected in infants presenting with heart failure in the setting of left ventricular systolic dysfunction and associated mitral regurgitation from papillary muscle ischemia. Adults with ALCAPA may present with cardiac ischemic symptoms. Prompt diagnosis with echocardiography and cross-sectional chest imaging is important to guide surgical intervention and improve the patients' survival and prognosis. The goal of surgery is to establish a dual-coronary system with mid-term results revealing progressive recovery of left ventricular function and improvement in mitral regurgitation. Patients with ALCAPA should maintain life-long follow-up with a cardiologist with congenital heart disease expertise for surveillance of post-operative complications.
Keywords: adult congenital heart disease; anomalous coronary artery; anomalous left coronary artery from the pulmonary artery (ALCAPA).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Surgical management of anomalous origin of coronary artery from pulmonary artery.Indian J Thorac Cardiovasc Surg. 2021 Jan;37(Suppl 1):131-143. doi: 10.1007/s12055-021-01147-8. Epub 2021 Jan 28. Indian J Thorac Cardiovasc Surg. 2021. PMID: 33526963 Free PMC article.
-
Anomalous Left Coronary Artery from Pulmonary Artery: An Important Cause of Ischemic Mitral Regurgitation in Children.Cureus. 2019 Apr 12;11(4):e4441. doi: 10.7759/cureus.4441. Cureus. 2019. PMID: 31245227 Free PMC article.
-
Two congenital coronary abnormalities affecting heart function: anomalous origin of the left coronary artery from the pulmonary artery and congenital left main coronary artery atresia.Chin Med J (Engl). 2014;127(21):3724-31. Chin Med J (Engl). 2014. PMID: 25382327
-
The management of the older adult patient with anomalous left coronary artery from the pulmonary artery syndrome: a presentation of two cases and review of the literature.Congenit Heart Dis. 2014 Nov-Dec;9(6):E185-94. doi: 10.1111/chd.12125. Epub 2013 Aug 18. Congenit Heart Dis. 2014. PMID: 23953779 Review.
-
Late complications after Takeuchi repair of anomalous left coronary artery from the pulmonary artery: case series and review of literature.Pediatr Cardiol. 2012 Oct;33(7):1115-23. doi: 10.1007/s00246-012-0260-5. Epub 2012 Mar 22. Pediatr Cardiol. 2012. PMID: 22438016 Review.
Cited by
-
Midterm outcome after surgical correction of an anomaly of the left coronary artery from the pulmonary artery.J Cardiothorac Surg. 2024 Sep 3;19(1):512. doi: 10.1186/s13019-024-02981-8. J Cardiothorac Surg. 2024. PMID: 39227974 Free PMC article.
-
Pulmonary hypertension associated with anomalous left coronary artery originating from the pulmonary artery.ESC Heart Fail. 2025 Feb;12(1):717-722. doi: 10.1002/ehf2.15094. Epub 2024 Sep 23. ESC Heart Fail. 2025. PMID: 39314034 Free PMC article. No abstract available.
-
Adult-type anomalous origin of the left coronary artery from the pulmonary artery and right coronary-right atrial fistula: a case report.BMC Cardiovasc Disord. 2024 Jan 5;24(1):31. doi: 10.1186/s12872-023-03686-x. BMC Cardiovasc Disord. 2024. PMID: 38183012 Free PMC article.
-
Concurrent finding of rheumatic severe mitral regurgitation and anomalous left coronary artery from the pulmonary artery (ALCAPA) in a 23-year-old patient consulting for ventricular tachycardia: A case report and a review of the literature.Int J Cardiol Congenit Heart Dis. 2024 Nov 20;19:100553. doi: 10.1016/j.ijcchd.2024.100553. eCollection 2025 Mar. Int J Cardiol Congenit Heart Dis. 2024. PMID: 39926121 Free PMC article.
-
The Winding Road to Dyspnea: A Case Report of an Unusual Presentation of Anomalous Left Coronary Artery from the Pulmonary Artery.Reports (MDPI). 2024 Dec 12;7(4):114. doi: 10.3390/reports7040114. Reports (MDPI). 2024. PMID: 40757711 Free PMC article.
References
-
- Boutsikou M., Shore D., Li W., Rubens M., Pijuan A., Gatzoulis M.A., Babu-Narayan S.V. Anomalous left coronary artery from the pulmonary artery (ALCAPA) diagnosed in adulthood: Varied clinical presentation, therapeutic approach, and outcome. Int. J. Cardiol. 2018;261:49–53. doi: 10.1016/j.ijcard.2018.02.082. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
