

PEAL Score to Predict the Mortality Risk of Cardiogenic Shock in the Emergency Department: An Observational Study
- PMID: 38003929
- PMCID: PMC10672116
- DOI: 10.3390/jpm13111614
PEAL Score to Predict the Mortality Risk of Cardiogenic Shock in the Emergency Department: An Observational Study
Abstract
Background: The in-hospital mortality of cardiogenic shock (CS) remains high (28% to 45%). As a result, several studies developed prediction models to assess the mortality risk and provide guidance on treatment, including CardShock and IABP-SHOCK II scores, which performed modestly in external validation studies, reflecting the heterogeneity of the CS populations. Few articles established predictive scores of CS based on Asian people with a higher burden of comorbidities than Caucasians. We aimed to describe the clinical characteristics of a contemporary Asian population with CS, identify risk factors, and develop a predictive scoring model.
Methods: A retrospective observational study was conducted between 2014 and 2019 to collect the patients who presented with all-cause CS in the emergency department of a single medical center in Taiwan. We divided patients into subgroups of CS related to acute myocardial infarction (AMI-CS) or heart failure (HF-CS). The outcome was all-cause 30-day mortality. We built the prediction model based on the hazard ratio of significant variables, and the cutoff point of each predictor was determined using the Youden index. We also assessed the discrimination ability of the risk score using the area under a receiver operating characteristic curve.
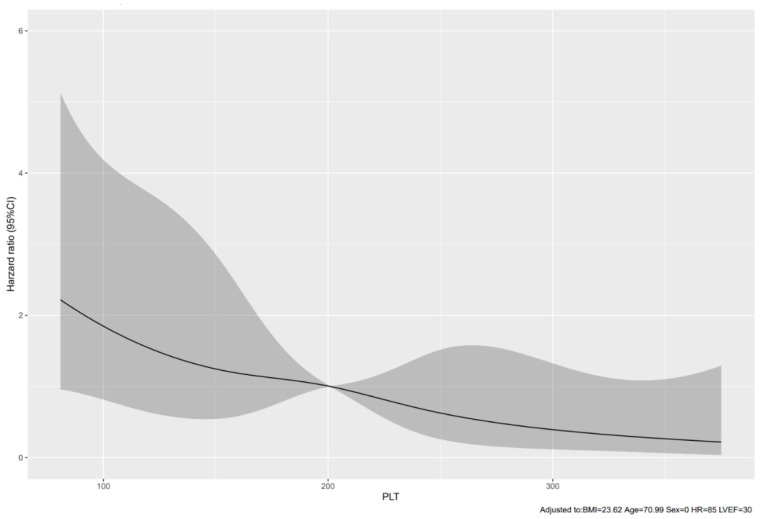
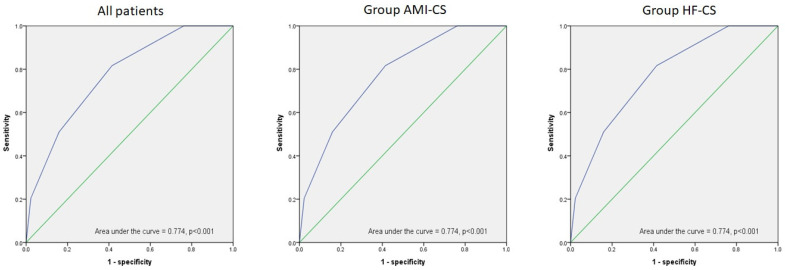
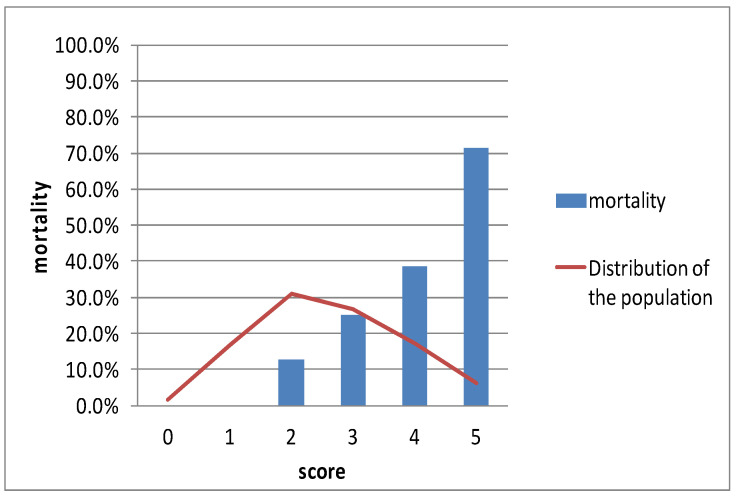
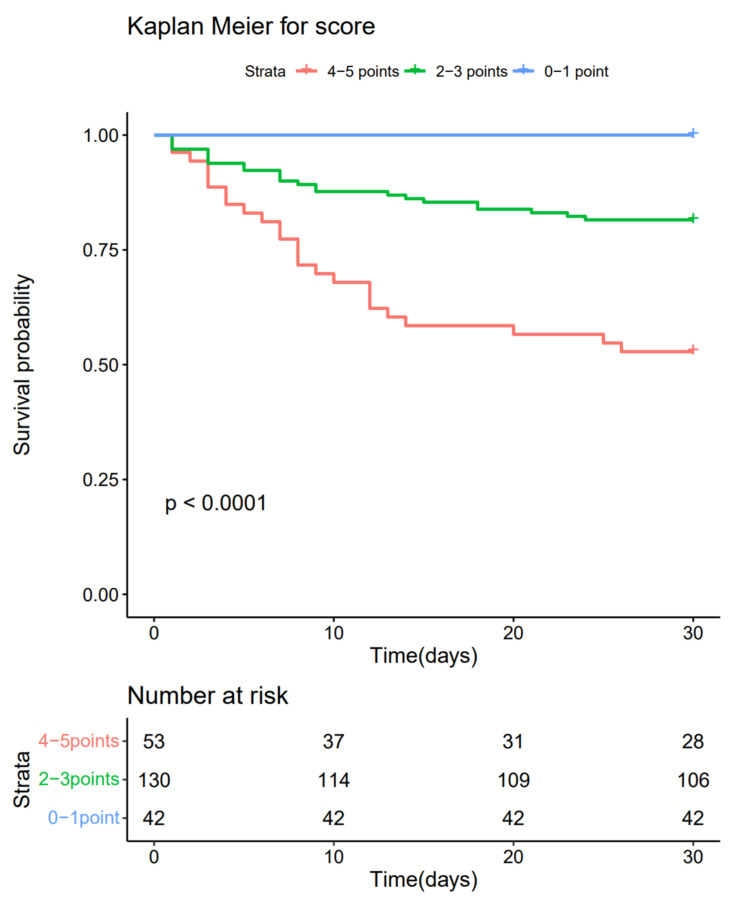
Results: We enrolled 225 patients with CS. One hundred and seven patients (47.6%) were due to AMI-CS, and ninety-eight patients among them received reperfusion therapy. Forty-nine patients (21.8%) eventually died within 30 days. Fifty-three patients (23.55%) presented with platelet counts < 155 × 103/μL, which were negatively associated with a 30-day mortality of CS in the restrictive cubic spline plot, even within the normal range of platelet counts. We identified four predictors: platelet counts < 200 × 103/μL (HR 2.574, 95% CI 1.379-4.805, p = 0.003), left ventricular ejection fraction (LVEF) < 40% (HR 2.613, 95% CI 1.020-6.692, p = 0.045), age > 71 years (HR 2.452, 95% CI 1.327-4.531, p = 0.004), and lactate > 2.7 mmol/L (HR 1.967, 95% CI 1.069-3.620, p = 0.030). The risk score ended with a maximum of 5 points and showed an AUC (95% CI) of 0.774 (0.705-0.843) for all patients, 0.781 (0.678-0.883), and 0.759 (0.662-0.855) for AMI-CS and HF-CS sub-groups, respectively, all p < 0.001.
Conclusions: Based on four parameters, platelet counts, LVEF, age, and lactate (PEAL), this model showed a good predictive performance for all-cause mortality at 30 days in the all patients, AMI-CS, and HF-CS subgroups. The restrictive cubic spline plot showed a significantly negative correlation between initial platelet counts and 30-day mortality risk in the AMI-CS and HF-CS subgroups.
Keywords: acute myocardial infarction; cardiogenic shock; mortality risk; platelet counts; score.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Cardiogenic shock mortality according to Aetiology in a Mediterranean cohort: Results from the Shock-CAT study.ESC Heart Fail. 2025 Apr;12(2):1336-1345. doi: 10.1002/ehf2.15148. Epub 2024 Nov 25. ESC Heart Fail. 2025. PMID: 39587711 Free PMC article.
-
The prognostic value of admission D-dimer level in patients with cardiogenic shock after acute myocardial infarction.Front Cardiovasc Med. 2023 Jan 9;9:1083881. doi: 10.3389/fcvm.2022.1083881. eCollection 2022. Front Cardiovasc Med. 2023. PMID: 36698952 Free PMC article.
-
Early risk stratification in patients with cardiogenic shock irrespective of the underlying cause - the Cardiogenic Shock Score.Eur J Heart Fail. 2022 Apr;24(4):657-667. doi: 10.1002/ejhf.2449. Epub 2022 Feb 14. Eur J Heart Fail. 2022. PMID: 35119176
-
Timing of mechanical circulatory support during primary angioplasty in acute myocardial infarction and cardiogenic shock: Systematic review and meta-analysis.Catheter Cardiovasc Interv. 2022 Mar;99(4):998-1005. doi: 10.1002/ccd.30137. Epub 2022 Feb 19. Catheter Cardiovasc Interv. 2022. PMID: 35182020
-
Artificial Intelligence in the Early Prediction of Cardiogenic Shock in Acute Heart Failure or Myocardial Infarction Patients: A Systematic Review and Meta-Analysis.Cureus. 2023 Dec 12;15(12):e50395. doi: 10.7759/cureus.50395. eCollection 2023 Dec. Cureus. 2023. PMID: 38213372 Free PMC article. Review.
Cited by
-
Mitochondrial autophagy-related lncRNAs as prognostic biomarkers and therapeutic targets in gastric adenocarcinoma.Discov Oncol. 2025 Mar 8;16(1):283. doi: 10.1007/s12672-025-02042-z. Discov Oncol. 2025. PMID: 40056287 Free PMC article.
References
-
- Helgestad O.K.L., Josiassen J., Hassager C., Jensen L.O., Holmvang L., Sørensen A., Frydland M., Lassen A.T., Udesen N.L.J., Schmidt H., et al. Temporal trends in incidence and patient characteristics in CS following acute myocardial infarction from 2010 to 2017: A Danish cohort study. Eur. J. Heart Fail. 2019;21:1370–1378. doi: 10.1002/ejhf.1566. - DOI - PubMed
-
- van Diepen S., Katz J.N., Albert N.M., Henry T.D., Jacobs A.K., Kapur N.K., Kilic A., Menon V., Ohman E.M., Sweitzer N.K., et al. Contemporary Management of CS: A Scientific Statement From the American Heart Association. Circulation. 2017;136:e232–e268. doi: 10.1161/CIR.0000000000000525. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
