

Cardiac Magnetic Resonance Left Ventricular Filling Pressure Is Associated with NT-proBNP in Patients with New Onset Heart Failure
- PMID: 38003973
- PMCID: PMC10673394
- DOI: 10.3390/medicina59111924
Cardiac Magnetic Resonance Left Ventricular Filling Pressure Is Associated with NT-proBNP in Patients with New Onset Heart Failure
Abstract
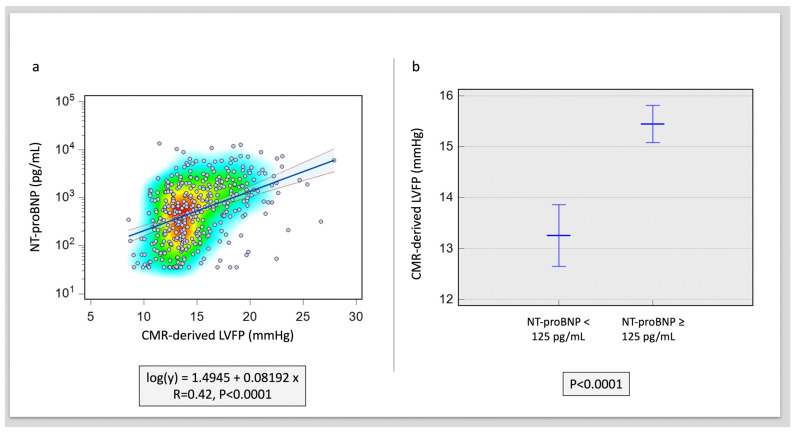
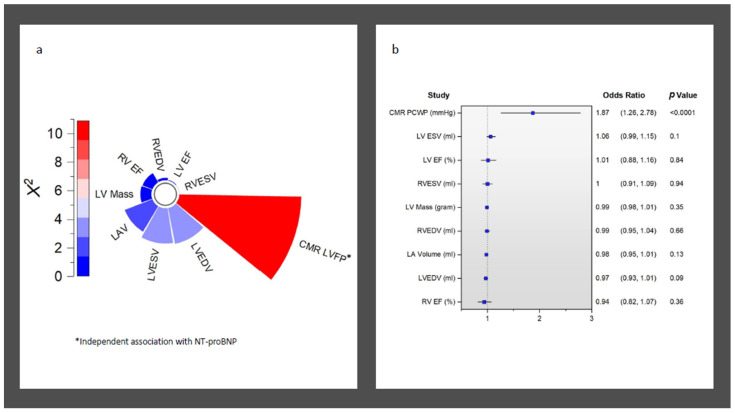
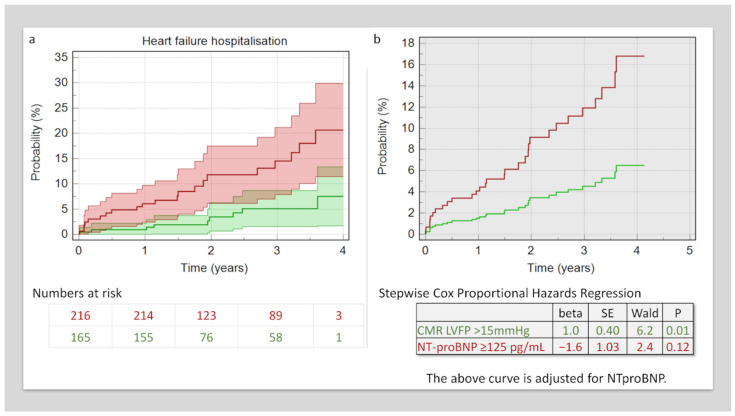
Background and Objectives: Cardiovascular magnetic resonance (CMR) is emerging as an important imaging tool for sub-phenotyping and estimating left ventricular (LV) filling pressure (LVFP). The N-terminal prohormone of B-type natriuretic peptide (NT-proBNP) is released from cardiac myocytes in response to mechanical load and wall stress. This study sought to investigate if CMR-derived LVFP is associated with the serum levels of NT-proBNP and, in addition, if it provides any incremental prognostic value in heart failure (HF). Materials and Methods: This study recruited 380 patients diagnosed with HF who underwent same-day CMR and clinical assessment between February 2018 and January 2020. CMR-derived LVFP was calculated, as previously, from long- and short-axis cines. During CMR assessment, serum NT-proBNP was measured. The pathological cut-offs were defined as follows: NT-proBNP ≥ 125 pg/mL and CMR LVFP > 15 mmHg. The incidence of HF hospitalisation was treated as a clinical outcome. Results: In total, 305 patients had NT-proBNP ≥ 125 pg/mL. Patients with raised NT-proBNP were older (54 ± 14 vs. 64 ± 11 years, p < 0.0001). Patients with raised NT-proBNP had higher LV volumes and mass. In addition, CMR LVFP was higher in patients with raised NT-proBNP (13.2 ± 2.6 vs. 15.4 ± 3.2 mmHg, p < 0.0001). The serum levels of NT-proBNP were associated with CMR-derived LVFP (R = 0.42, p < 0.0001). In logistic regression analysis, this association between NT-proBNP and CMR LVFP was independent of all other CMR variables, including LV ejection fraction, LV mass, and left atrial volume (coefficient = 2.02, p = 0.002). CMR LVFP demonstrated an independent association with the incidence of HF hospitalisation above NT-proBNP (hazard ratio 2.7, 95% confidence interval 1.2 to 6, p = 0.01). Conclusions: A CMR-modelled LVFP is independently associated with serum NT-proBNP levels. Importantly, it provides an incremental prognostic value over and above serum NT-proBNP levels.
Keywords: CMR; MRI; diastole; heart failure; left ventricular end-diastolic pressure.
Conflict of interest statement
P.G. is a clinical advisor for Pie Medical Imaging and Medis Medical Imaging. All other authors have no conflict of interest to declare.
Figures
Similar articles
-
CMR Left Ventricular Filling Pressure Exhibits Strong Haemodynamic Relevance and Outperforms Echocardiography in Multimodal Heart Failure Assessment.J Cardiovasc Dev Dis. 2025 Jun 27;12(7):250. doi: 10.3390/jcdd12070250. J Cardiovasc Dev Dis. 2025. PMID: 40710774 Free PMC article.
-
Cardiac magnetic resonance left ventricular filling pressure is linked to symptoms, signs and prognosis in heart failure.ESC Heart Fail. 2023 Oct;10(5):3067-3076. doi: 10.1002/ehf2.14499. Epub 2023 Aug 19. ESC Heart Fail. 2023. PMID: 37596895 Free PMC article.
-
Cardiac magnetic resonance identifies raised left ventricular filling pressure: prognostic implications.Eur Heart J. 2022 Jul 7;43(26):2511-2522. doi: 10.1093/eurheartj/ehac207. Eur Heart J. 2022. PMID: 35512290 Free PMC article.
-
Strategic multimodal non-invasive assessment of cardiac performance in patients with heart failure.ESC Heart Fail. 2023 Aug;10(4):2567-2576. doi: 10.1002/ehf2.14425. Epub 2023 Jun 13. ESC Heart Fail. 2023. PMID: 37312276 Free PMC article.
-
Plasma N-terminal protype-B natriuretic peptide and restrictive mitral flow to risk-stratify patients with stage B heart failure.Clin Cardiol. 2009 Dec;32(12):711-7. doi: 10.1002/clc.20617. Clin Cardiol. 2009. PMID: 20027664 Free PMC article.
Cited by
-
Risk factors and establishment of a nomogram model for pulmonary arterial hypertension complicated by acute exacerbation of chronic obstructive pulmonary disease.Am J Transl Res. 2025 May 15;17(5):3917-3927. doi: 10.62347/XMTE6690. eCollection 2025. Am J Transl Res. 2025. PMID: 40535618 Free PMC article.
-
Cardiac MRI-derived mean right atrial pressure and its prognostic importance.Open Heart. 2025 Jun 22;12(1):e003216. doi: 10.1136/openhrt-2025-003216. Open Heart. 2025. PMID: 40550572 Free PMC article.
-
CMR Left Ventricular Filling Pressure Exhibits Strong Haemodynamic Relevance and Outperforms Echocardiography in Multimodal Heart Failure Assessment.J Cardiovasc Dev Dis. 2025 Jun 27;12(7):250. doi: 10.3390/jcdd12070250. J Cardiovasc Dev Dis. 2025. PMID: 40710774 Free PMC article.
-
Validation of Left Atrial Volume Correction for Single Plane Method on Four-Chamber Cine Cardiac MRI.Tomography. 2024 Mar 25;10(4):459-470. doi: 10.3390/tomography10040035. Tomography. 2024. PMID: 38668393 Free PMC article.
References
-
- Hunt S.A., Abraham W.T., Chin M.H., Feldman A.M., Francis G.S., Ganiats T.G., Jessup M., Konstam M.A., Mancini D.M., Michl K., et al. 2009 Focused Update Incorporated Into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the International Society for Heart and Lung Transplantation. J. Am. Coll. Cardiol. 2009;53:e391–e479. - PubMed
-
- Lancellotti P., Galderisi M., Edvardsen T., Donal E., Goliasch G., Cardim N., Magne J., Laginha S., Hagendorff A., Haland T.F., et al. Echo-Doppler estimation of left ventricular filling pressure: Results of the multicentre EACVI Euro-Filling study. Eur. Heart J. Cardiovasc. Imaging. 2017;18:961–968. doi: 10.1093/ehjci/jex067. - DOI - PubMed
-
- Writing Committee Members. Quiñones M.A., Douglas P.S., Foster E., Gorcsan J., Lewis J.F., Pearlman A.S., Rychik J., Salcedo E.E., Seward J.B., et al. American College of Cardiology/American Heart Association clinical competence statement on echocardiography: A report of the American College of Cardiology/American Heart Association/American College of Physicians—American Society of Internal Medicine Task Force on Clinical Competence. Circulation. 2003;107:1068–1089. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
