

The Left Atrial Area Derived Cardiovascular Magnetic Resonance Left Ventricular Filling Pressure Equation Shows Superiority over Integrated Echocardiography
- PMID: 38004001
- PMCID: PMC10672763
- DOI: 10.3390/medicina59111952
The Left Atrial Area Derived Cardiovascular Magnetic Resonance Left Ventricular Filling Pressure Equation Shows Superiority over Integrated Echocardiography
Abstract
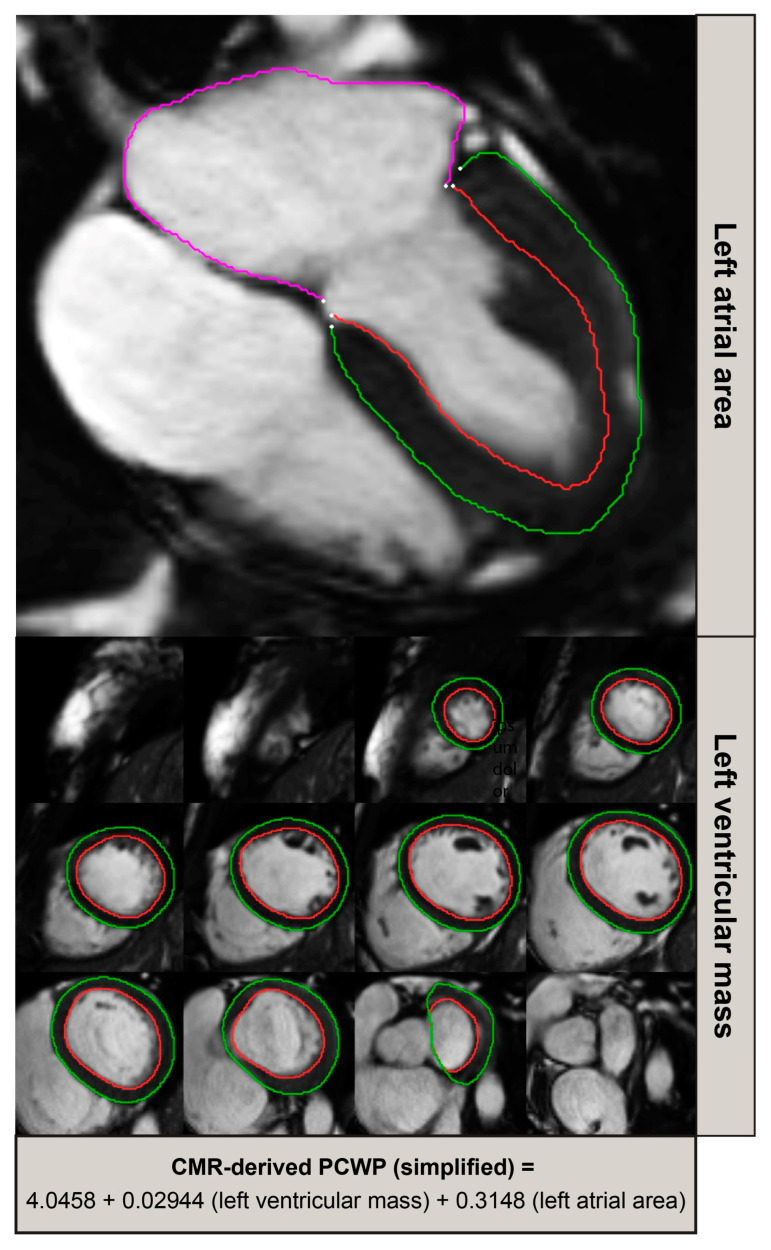
Background and objectives: Evaluating left ventricular filling pressure (LVFP) plays a crucial role in diagnosing and managing heart failure (HF). While traditional assessment methods involve multi-parametric transthoracic echocardiography (TTE) or right heart catheterisation (RHC), cardiovascular magnetic resonance (CMR) has emerged as a valuable diagnostic tool in HF. This study aimed to assess a simple CMR-derived model to estimate pulmonary capillary wedge pressure (PCWP) in a cohort of patients with suspected or proven heart failure and to investigate its performance in risk-stratifying patients. Materials and methods: A total of 835 patients with breathlessness were evaluated using RHC and CMR and split into derivation (85%) and validation cohorts (15%). Uni-variate and multi-variate linear regression analyses were used to derive a model for PCWP estimation using CMR. The model's performance was evaluated by comparing CMR-derived PCWP with PCWP obtained from RHC. Results: A CMR-derived PCWP incorporating left ventricular mass and the left atrial area (LAA) demonstrated good diagnostic accuracy. The model correctly reclassified 66% of participants whose TTE was 'indeterminate' or 'incorrect' in identifying raised filling pressures. On survival analysis, the CMR-derived PCWP model was predictive for mortality (HR 1.15, 95% CI 1.04-1.28, p = 0.005), which was not the case for PCWP obtained using RHC or TTE. Conclusions: The simplified CMR-derived PCWP model provides an accurate and practical tool for estimating PCWP in patients with suspected or proven heart failure. Its predictive value for mortality suggests the ability to play a valuable adjunctive role in echocardiography, especially in cases with unclear echocardiographic assessment.
Keywords: cardiovascular magnetic resonance; echocardiography; filling pressure; haemodynamic assessment; heart failure.
Conflict of interest statement
P.G. is a clinical advisor for Pie Medical Imaging and Medis Medical Imaging. All other authors have no conflict of interest to declare.
Figures



References
-
- Pieske B., Tschöpe C., de Boer R.A., Fraser A.G., Anker S.D., Donal E., Edelmann F., Fu M., Guazzi M., Lam C.S.P., et al. How to diagnose heart failure with preserved ejection fraction: The HFA–PEFF diagnostic algorithm: A consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC) Eur. Heart J. 2019;40:3297–3317. doi: 10.1093/eurheartj/ehz641. - DOI - PubMed
-
- Lancellotti P., Nkomo V.T., Badano L.P., Bergler-Klein J., Bogaert J., Davin L., Cosyns B., Coucke P., Dulgheru R., Edvardsen T., et al. Expert consensus for multi-modality imaging evaluation of cardiovascular complications of radiotherapy in adults: A report from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging. 2013;14:721–740. doi: 10.1093/ehjci/jet123. - DOI - PubMed
-
- Nagesh S.F., Smiseth O.A., Appleton C.P., Byrd B.F., Dokainish H., Edvardsen T., Flachskampf F.A., Gillebert T.C., Klein A.L., Lancellotti P., et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2016;29:277–314. doi: 10.1016/j.echo.2016.01.011. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
