

Stable Gastric Pentadecapeptide BPC 157 Therapy: Effect on Reperfusion Following Maintained Intra-Abdominal Hypertension (Grade III and IV) in Rats
- PMID: 38004420
- PMCID: PMC10675657
- DOI: 10.3390/ph16111554
Stable Gastric Pentadecapeptide BPC 157 Therapy: Effect on Reperfusion Following Maintained Intra-Abdominal Hypertension (Grade III and IV) in Rats
Abstract
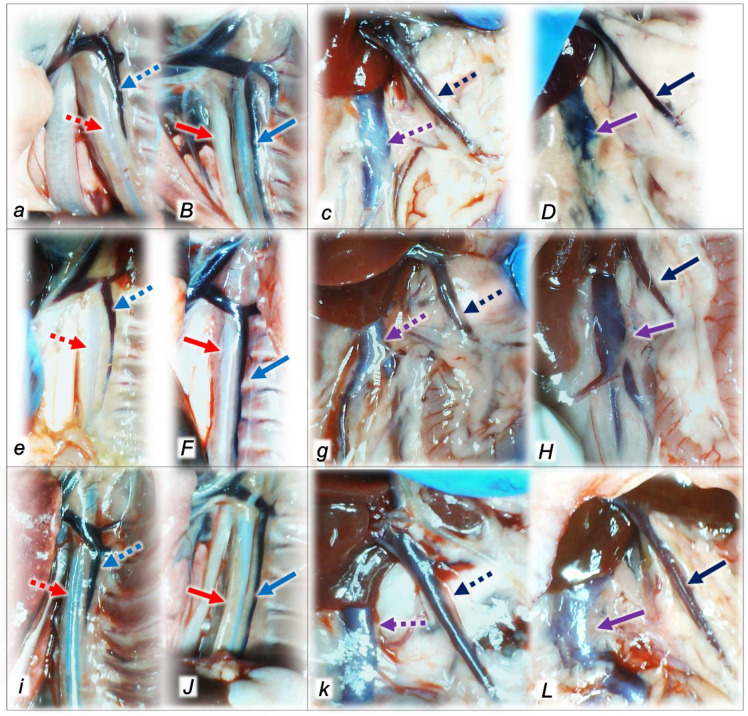
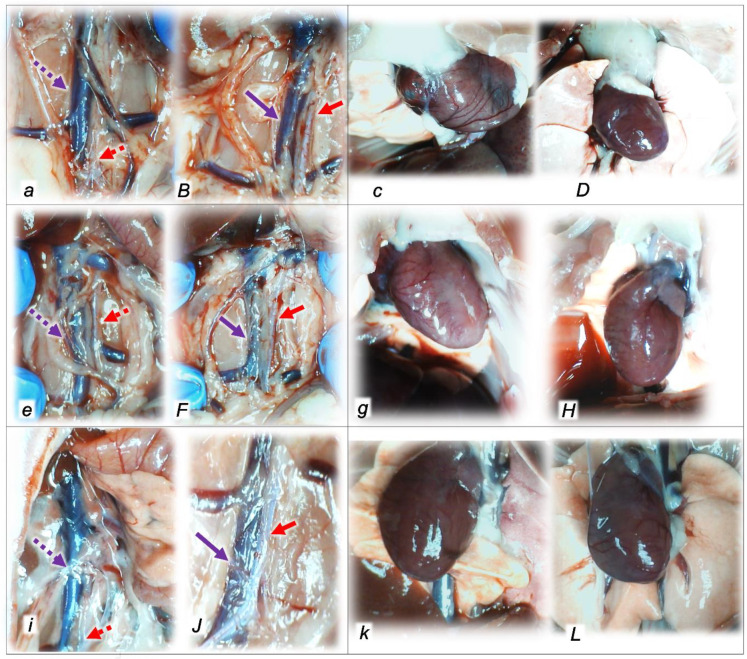
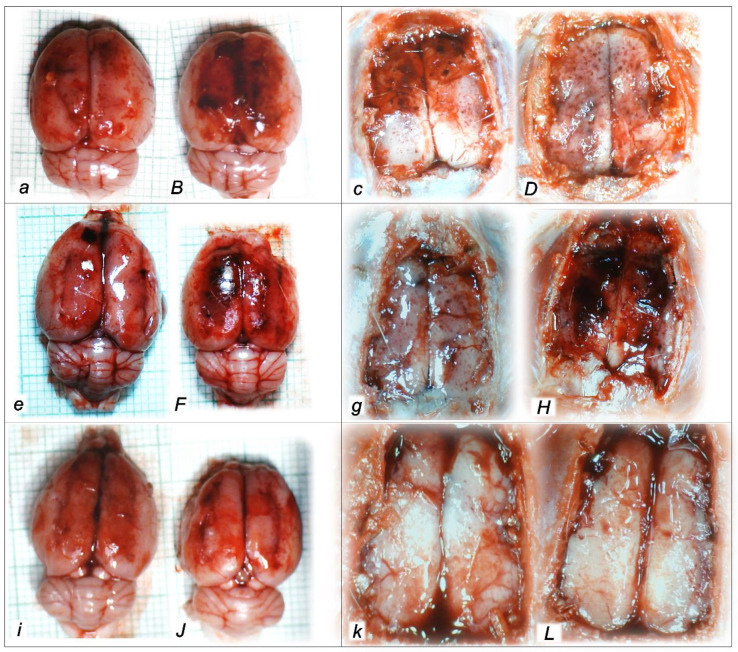
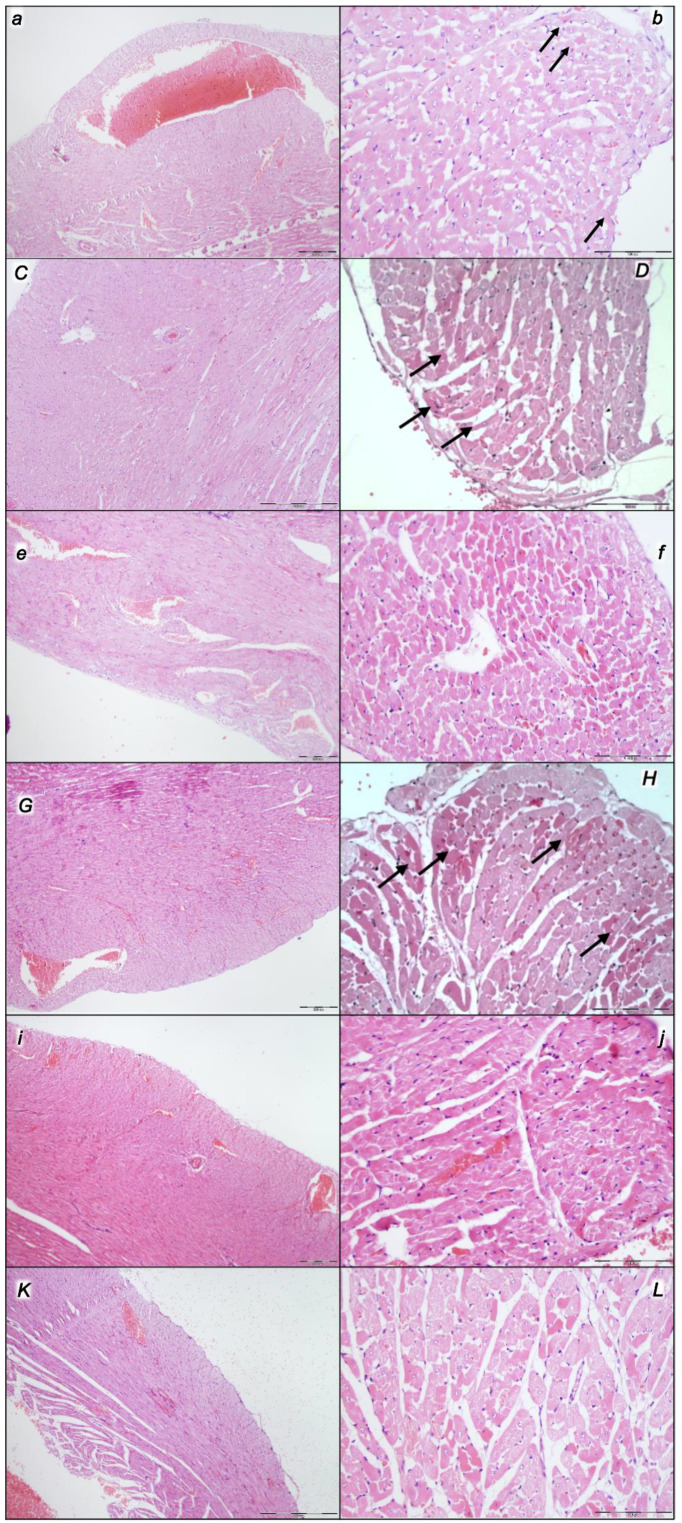
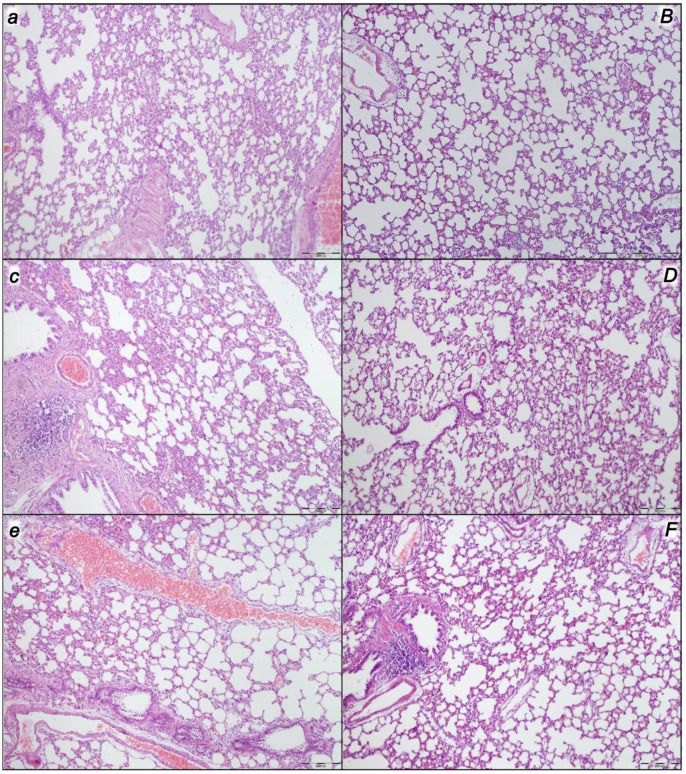
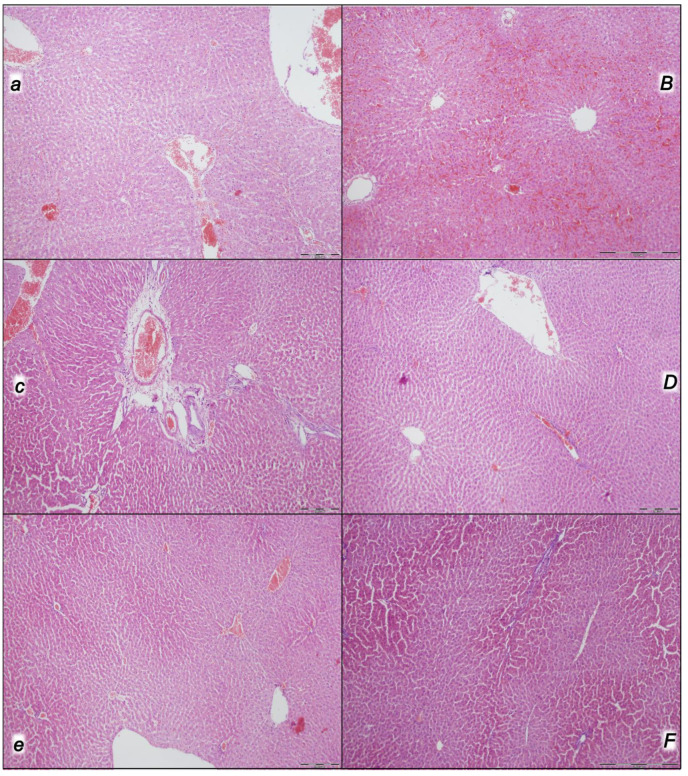
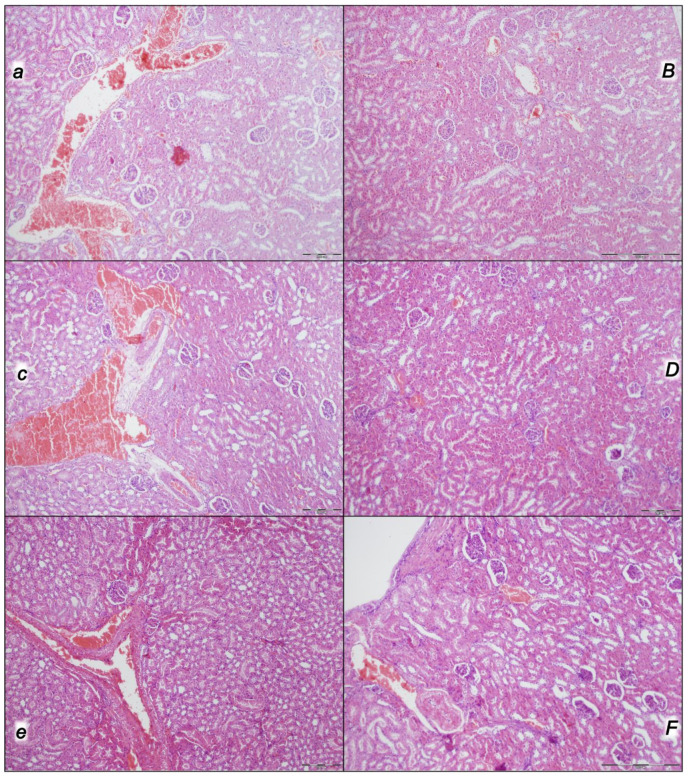
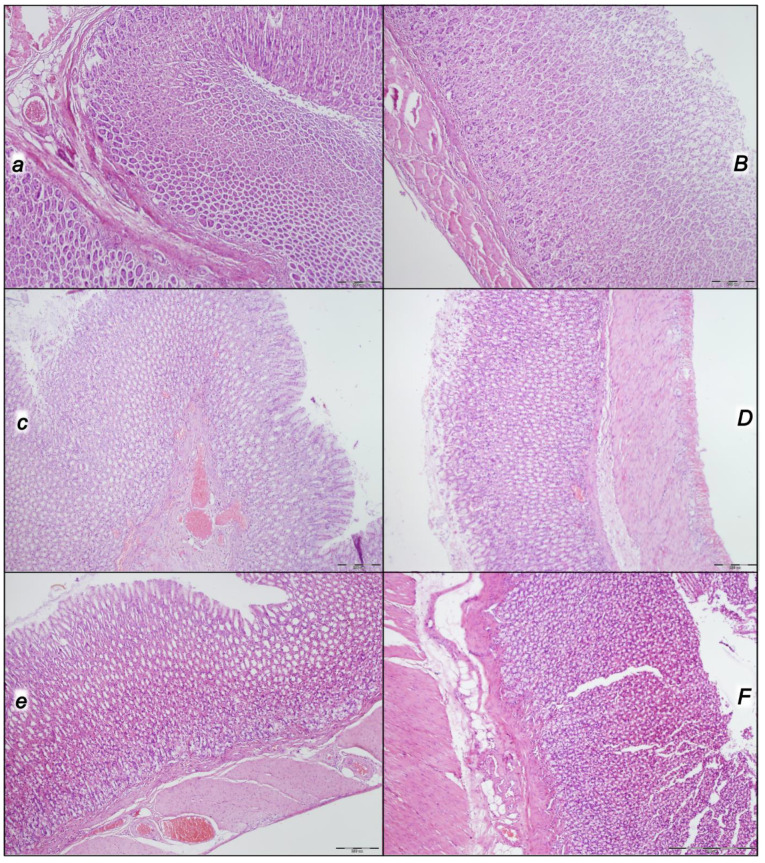
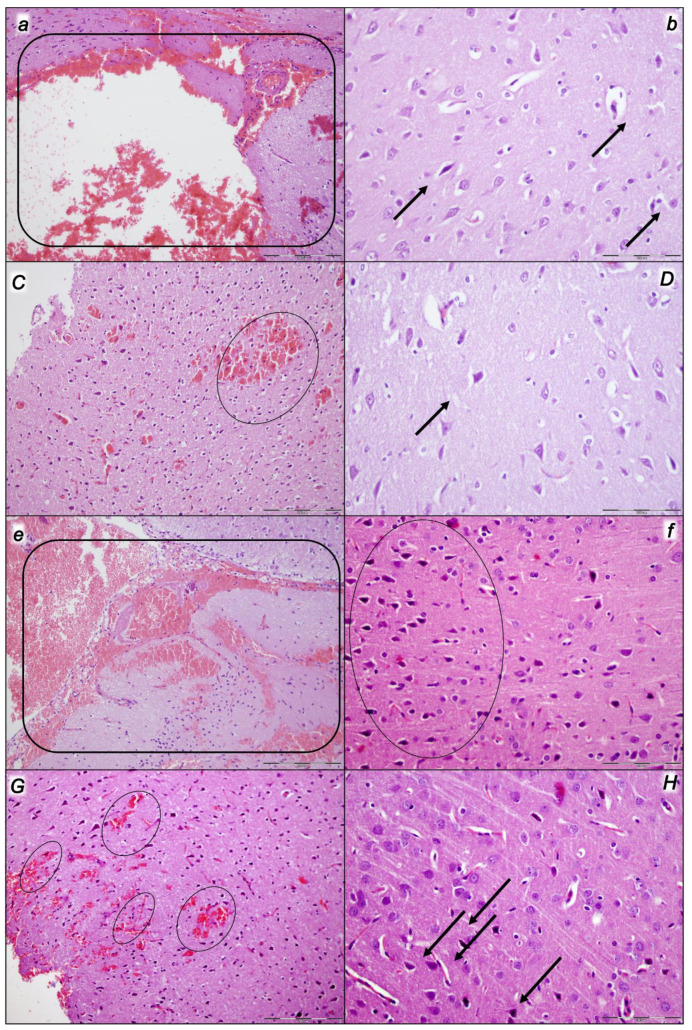
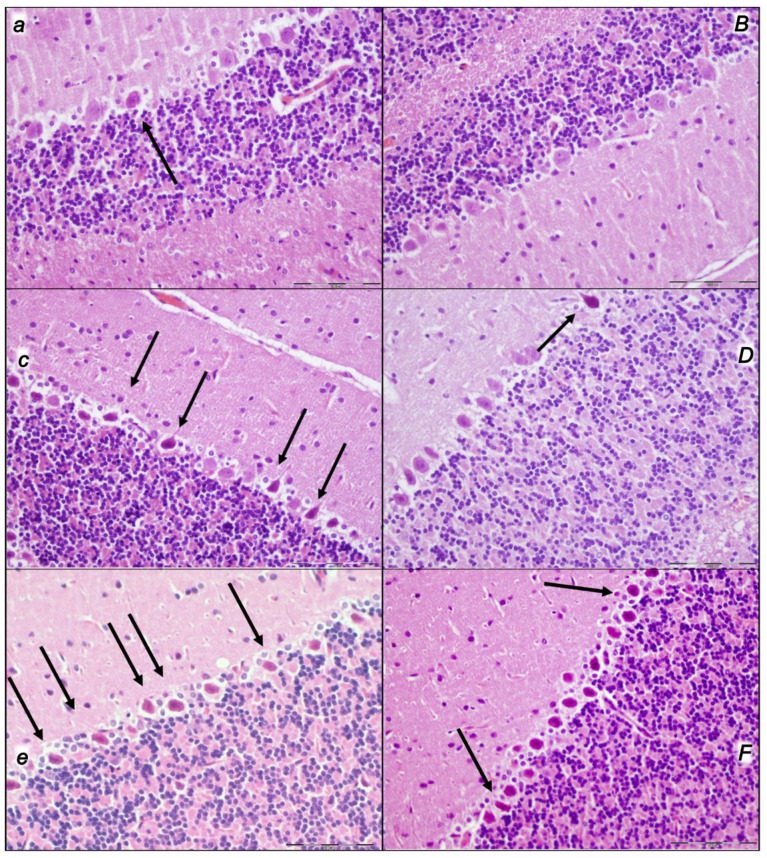
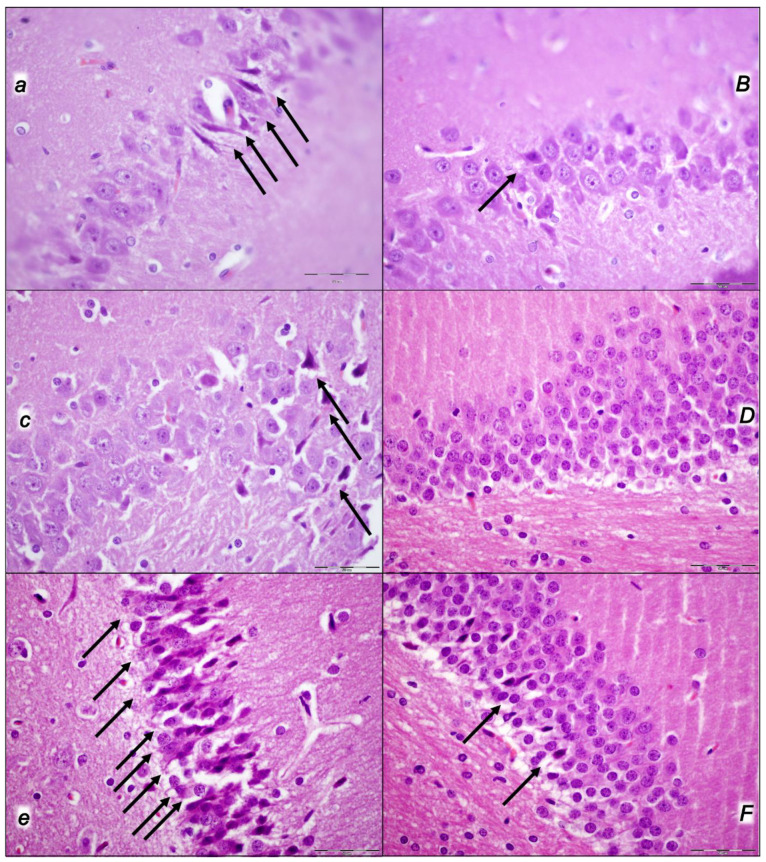
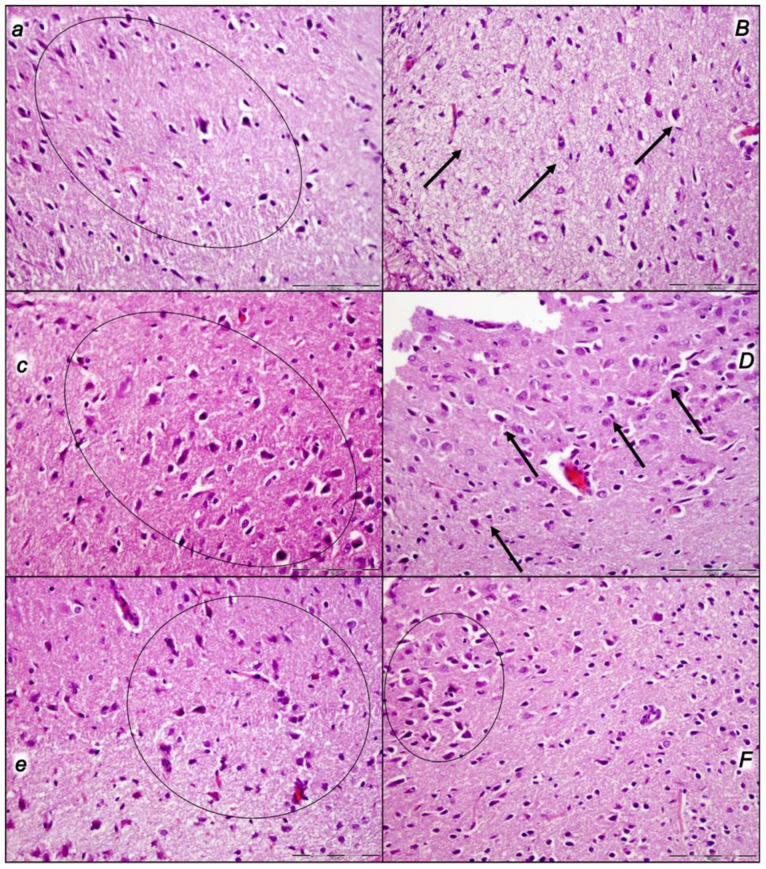
Given in reperfusion, the use of stable gastric pentadecapeptide BPC 157 is an effective therapy in rats. It strongly counteracted, as a whole, decompression/reperfusion-induced occlusion/occlusion-like syndrome following the worst circumstances of acute abdominal compartment and intra-abdominal hypertension, grade III and grade IV, as well as compression/ischemia-occlusion/occlusion-like syndrome. Before decompression (calvariectomy, laparotomy), rats had long-lasting severe intra-abdominal hypertension, grade III (25 mmHg/60 min) (i) and grade IV (30 mmHg/30 min; 40 mmHg/30 min) (ii/iii), and severe occlusion/occlusion-like syndrome. Further worsening was caused by reperfusion for 60 min (i) or 30 min (ii/iii). Severe vascular and multiorgan failure (brain, heart, liver, kidney, and gastrointestinal lesions), widespread thrombosis (peripherally and centrally) severe arrhythmias, intracranial (superior sagittal sinus) hypertension, portal and caval hypertension, and aortal hypotension were aggravated. Contrarily, BPC 157 therapy (10 µg/kg, 10 ng/kg sc) given at 3 min reperfusion times eliminated/attenuated venous hypertension (intracranial (superior sagittal sinus), portal, and caval) and aortal hypotension and counteracted the increases in organ lesions and malondialdehyde values (blood ˃ heart, lungs, liver, kidney ˃ brain, gastrointestinal tract). Vascular recovery promptly occurred (i.e., congested inferior caval and superior mesenteric veins reversed to the normal vessel presentation, the collapsed azygos vein reversed to a fully functioning state, the inferior caval vein-superior caval vein shunt was recovered, and direct blood delivery returned). BPC 157 therapy almost annihilated thrombosis and hemorrhage (i.e., intracerebral hemorrhage) as proof of the counteracted general stasis and Virchow triad circumstances and reorganized blood flow. In conclusion, decompression/reperfusion-induced occlusion/occlusion-like syndrome counteracted by BPC 157 therapy in rats is likely for translation in patients. It is noteworthy that by rapidly counteracting the reperfusion course, it also reverses previous ischemia-course lesions, thus inducing complete recovery.
Keywords: occlusion/occlusion-like syndrome; prime acute abdominal compartment; reperfusion; stable gastric pentadecapeptide BPC 157 therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
New studies with stable gastric pentadecapeptide protecting gastrointestinal tract. significance of counteraction of vascular and multiorgan failure of occlusion/occlusion-like syndrome in cytoprotection/organoprotection.Inflammopharmacology. 2024 Oct;32(5):3119-3161. doi: 10.1007/s10787-024-01499-8. Epub 2024 Jul 9. Inflammopharmacology. 2024. PMID: 38980576 Review.
-
Acute Compartment Syndrome and Intra-Abdominal Hypertension, Decompression, Current Pharmacotherapy, and Stable Gastric Pentadecapeptide BPC 157 Solution.Pharmaceuticals (Basel). 2025 Jun 10;18(6):866. doi: 10.3390/ph18060866. Pharmaceuticals (Basel). 2025. PMID: 40573261 Free PMC article. Review.
-
Stomach perforation-induced general occlusion/occlusion-like syndrome and stable gastric pentadecapeptide BPC 157 therapy effect.World J Gastroenterol. 2023 Jul 21;29(27):4289-4316. doi: 10.3748/wjg.v29.i27.4289. World J Gastroenterol. 2023. PMID: 37545637 Free PMC article.
-
Pentadecapeptide BPC 157 as Therapy for Inferior Caval Vein Embolization: Recovery of Sodium Laurate-Post-Embolization Syndrome in Rats.Pharmaceuticals (Basel). 2023 Oct 23;16(10):1507. doi: 10.3390/ph16101507. Pharmaceuticals (Basel). 2023. PMID: 37895979 Free PMC article.
-
Stable Gastric Pentadecapeptide BPC 157 Therapy for Primary Abdominal Compartment Syndrome in Rats.Front Pharmacol. 2021 Dec 13;12:718147. doi: 10.3389/fphar.2021.718147. eCollection 2021. Front Pharmacol. 2021. PMID: 34966273 Free PMC article.
Cited by
-
New studies with stable gastric pentadecapeptide protecting gastrointestinal tract. significance of counteraction of vascular and multiorgan failure of occlusion/occlusion-like syndrome in cytoprotection/organoprotection.Inflammopharmacology. 2024 Oct;32(5):3119-3161. doi: 10.1007/s10787-024-01499-8. Epub 2024 Jul 9. Inflammopharmacology. 2024. PMID: 38980576 Review.
-
Acute Compartment Syndrome and Intra-Abdominal Hypertension, Decompression, Current Pharmacotherapy, and Stable Gastric Pentadecapeptide BPC 157 Solution.Pharmaceuticals (Basel). 2025 Jun 10;18(6):866. doi: 10.3390/ph18060866. Pharmaceuticals (Basel). 2025. PMID: 40573261 Free PMC article. Review.
-
Stable Gastric Pentadecapeptide BPC 157 as a Therapy and Safety Key: A Special Beneficial Pleiotropic Effect Controlling and Modulating Angiogenesis and the NO-System.Pharmaceuticals (Basel). 2025 Jun 19;18(6):928. doi: 10.3390/ph18060928. Pharmaceuticals (Basel). 2025. PMID: 40573323 Free PMC article. Review.
-
The Stable Gastric Pentadecapeptide BPC 157 Pleiotropic Beneficial Activity and Its Possible Relations with Neurotransmitter Activity.Pharmaceuticals (Basel). 2024 Apr 3;17(4):461. doi: 10.3390/ph17040461. Pharmaceuticals (Basel). 2024. PMID: 38675421 Free PMC article. Review.
-
Stable Gastric Pentadecapeptide BPC 157 and Intestinal Anastomoses Therapy in Rats-A Review.Pharmaceuticals (Basel). 2024 Aug 17;17(8):1081. doi: 10.3390/ph17081081. Pharmaceuticals (Basel). 2024. PMID: 39204186 Free PMC article. Review.
References
-
- Sikiric P., Skrtic A., Gojkovic S., Krezic I., Zizek H., Lovric E., Sikiric S., Knezevic M., Strbe S., Milavic M., et al. Cytoprotective gastric pentadecapeptide BPC 157 resolves major vessel occlusion disturbances, ischemia-reperfusion injury following Pringle maneuver, and Budd-Chiari syndrome. World J. Gastroenterol. 2022;28:23–46. doi: 10.3748/wjg.v28.i1.23. - DOI - PMC - PubMed
-
- Sikiric P., Hahm K.B., Blagaic A.B., Tvrdeic A., Pavlov K.H., Petrovic A., Kokot A., Gojkovic S., Krezic I., Drmic D., et al. Stable gastric pentadecapeptide BPC 157, Robert’s stomach cytoprotection/adaptive cytoprotection/organoprotection, and Selye’s stress coping response: Progress, achievements, and the future. Gut Liver. 2020;14:153–167. doi: 10.5009/gnl18490. - DOI - PMC - PubMed
-
- Sikiric P., Rucman R., Turkovic B., Sever M., Klicek R., Radic B., Drmic D., Stupnisek M., Misic M., Vuletic L.B., et al. Novel cytoprotective mediator, stable gastric pentadecapeptide BPC 157. Vascular recruitment and gastrointestinal tract healing. Curr. Pharm. Des. 2018;24:1990–2001. doi: 10.2174/1381612824666180608101119. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
