

Metronidazole Treatment Failure and Persistent BV Lead to Increased Frequencies of Activated T- and Dendritic-Cell Subsets
- PMID: 38004655
- PMCID: PMC10673474
- DOI: 10.3390/microorganisms11112643
Metronidazole Treatment Failure and Persistent BV Lead to Increased Frequencies of Activated T- and Dendritic-Cell Subsets
Abstract
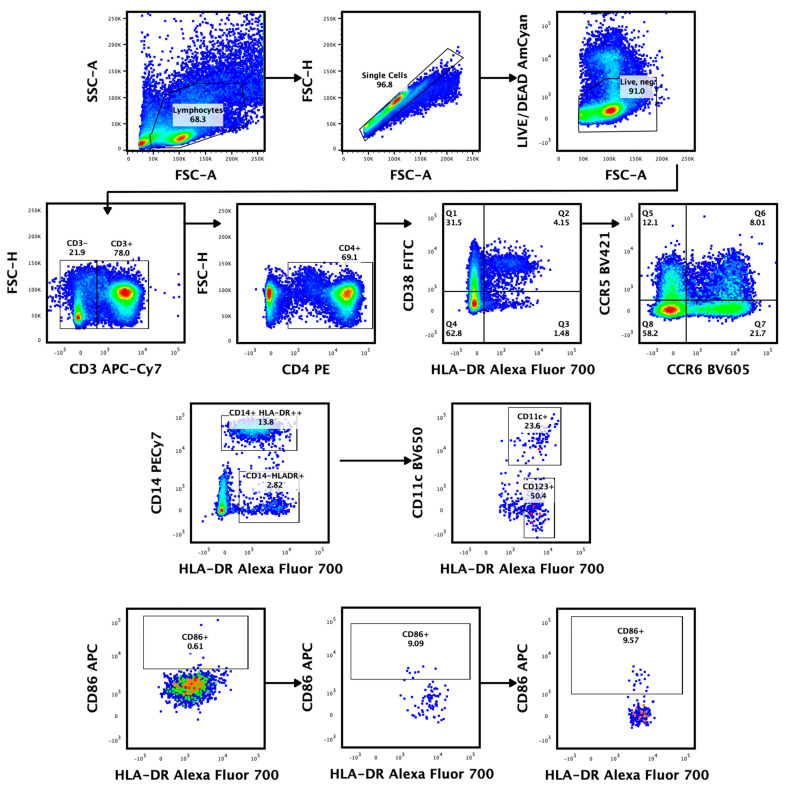
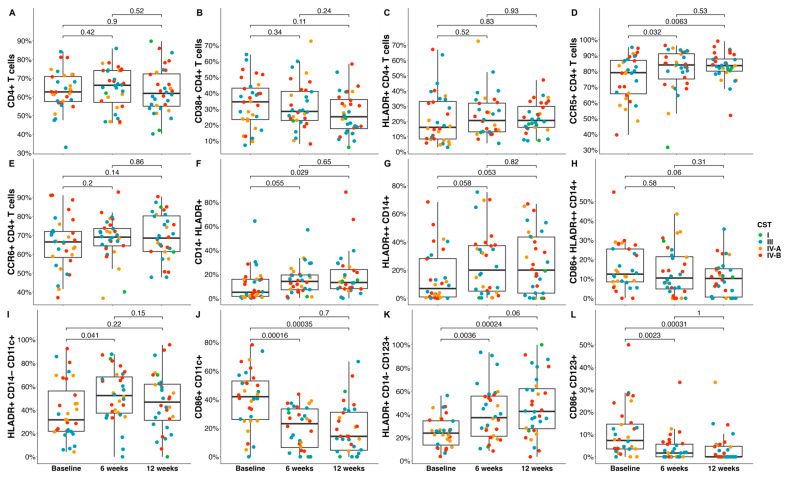
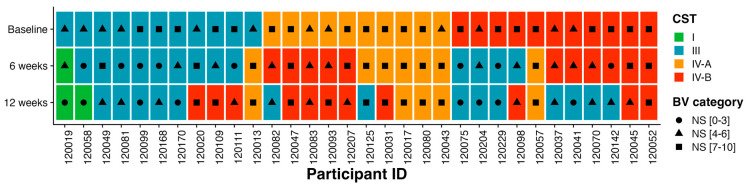
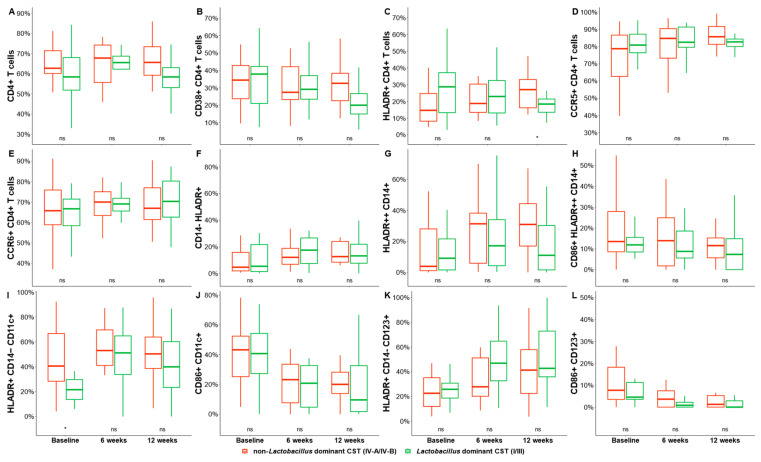
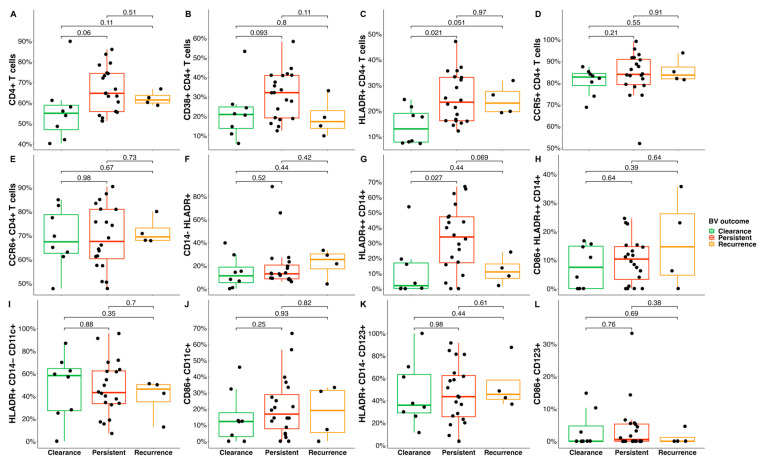
Metronidazole (MDZ) treatment failure and bacterial vaginosis (BV) recurrence rates are high among African women. This cohort study identified genital immune parameters associated with treatment response by comparing vaginal microbiota and immune cell frequencies in endocervical cytobrushes obtained from 32 South African women with symptomatic BV pre- and post-metronidazole treatment. Cervical T- and dendritic-cell subsets were phenotyped using multiparameter flow cytometry and the composition of vaginal microbial communities was characterized using 16S rRNA gene sequencing. MDZ treatment led to a modest decrease in the relative abundance of BV-associated bacteria, but colonization with Lactobacillus species (other than L. iners) was rare. At 6 and 12 weeks, MDZ-treated women had a significant increase in the frequencies of CCR5+ CD4+ T cells and plasmacytoid dendritic cells compared to the pre-treatment timepoint. In addition, MDZ non-responders had significantly higher frequencies of activated CD4 T cells and monocytes compared to MDZ responders. We conclude that MDZ treatment failure was characterized by an increased expression of activated T- and dendritic-cell subsets that may enhance HIV susceptibility. These data suggest the need to further assess the long-term impact of MDZ treatment on mucosal immune response and the vaginal microbiota.
Keywords: BV treatment; genital immune cells; vaginal microbiota.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
Similar articles
-
Temporal Changes in Vaginal Microbiota and Genital Tract Cytokines Among South African Women Treated for Bacterial Vaginosis.Front Immunol. 2021 Sep 14;12:730986. doi: 10.3389/fimmu.2021.730986. eCollection 2021. Front Immunol. 2021. PMID: 34594336 Free PMC article.
-
Impact of Standard Bacterial Vaginosis Treatment on the Genital Microbiota, Immune Milieu, and Ex Vivo Human Immunodeficiency Virus Susceptibility.Clin Infect Dis. 2019 May 2;68(10):1675-1683. doi: 10.1093/cid/ciy762. Clin Infect Dis. 2019. PMID: 30407498 Free PMC article.
-
Single-Molecule Approach to 16S rRNA for Vaginal Microbiome Signatures in Response to Metronidazole Treatment.Microbiol Spectr. 2023 Jun 15;11(3):e0170622. doi: 10.1128/spectrum.01706-22. Epub 2023 May 18. Microbiol Spectr. 2023. PMID: 37199621 Free PMC article.
-
Beyond bacterial vaginosis: vaginal lactobacilli and HIV risk.Microbiome. 2021 Dec 10;9(1):239. doi: 10.1186/s40168-021-01183-x. Microbiome. 2021. PMID: 34893070 Free PMC article. Review.
-
Optimizing the vaginal microbiome as a potential strategy to reduce heterosexual HIV transmission.J Intern Med. 2023 Apr;293(4):433-444. doi: 10.1111/joim.13600. Epub 2022 Dec 31. J Intern Med. 2023. PMID: 36544257 Review.
Cited by
-
Bacterial vaginosis associates with dysfunctional T cells and altered soluble immune factors in the cervicovaginal tract.J Clin Invest. 2025 Mar 25;135(10):e184609. doi: 10.1172/JCI184609. eCollection 2025 May 15. J Clin Invest. 2025. PMID: 40131862 Free PMC article.
-
The human vaginal microbiota: from clinical medicine to models to mechanisms.Curr Opin Microbiol. 2024 Feb;77:102422. doi: 10.1016/j.mib.2023.102422. Epub 2024 Jan 11. Curr Opin Microbiol. 2024. PMID: 38215548 Free PMC article. Review.
-
Effect of the vaginal live biotherapeutic LACTIN-V (Lactobacillus crispatus CTV-05) on vaginal microbiota and genital tract inflammation among women at high risk of HIV acquisition in South Africa: a phase 2, randomised, placebo-controlled trial.Lancet Microbe. 2025 Jun;6(6):101037. doi: 10.1016/j.lanmic.2024.101037. Epub 2025 Apr 4. Lancet Microbe. 2025. PMID: 40194532 Free PMC article. Clinical Trial.
-
Association between changes in genital immune markers and vaginal microbiome transitions in bacterial vaginosis.Sci Rep. 2025 Jan 28;15(1):3536. doi: 10.1038/s41598-025-88208-9. Sci Rep. 2025. PMID: 39875510 Free PMC article.
-
Bacterial vaginosis-driven changes in cervicovaginal immunity that expand the immunological hypothesis for increased HIV susceptibility.bioRxiv [Preprint]. 2025 Jan 14:2024.07.03.601916. doi: 10.1101/2024.07.03.601916. bioRxiv. 2025. PMID: 39005354 Free PMC article. Preprint.
References
-
- Shipitsyna E., Roos A., Datcu R., Hallen A., Fredlund H., Jensen J.S., Engstrand L., Unemo M. Composition of the vaginal microbiota in women of reproductive age—Sensitive and specific molecular diagnosis of bacterial vaginosis is possible? PLoS ONE. 2013;8:e60670. doi: 10.1371/journal.pone.0060670. - DOI - PMC - PubMed
-
- Bradshaw C.S., Vodstrcil L.A., Hocking J.S., Law M., Pirotta M., Garland S.M., De Guingand D., Morton A.N., Fairley C.K. Recurrence of bacterial vaginosis is significantly associated with posttreatment sexual activities and hormonal contraceptive use. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2013;56:777–786. doi: 10.1093/cid/cis1030. - DOI - PubMed
-
- Swidsinski A., Loening-Baucke V., Swidsinski S., Verstraelen H. Polymicrobial Gardnerella biofilm resists repeated intravaginal antiseptic treatment in a subset of women with bacterial vaginosis: A preliminary report. Arch. Gynecol. Obstet. 2015;291:605–609. doi: 10.1007/s00404-014-3484-1. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
