

Pediatric headache patient with cerebral abscesses: a brief review of the literature and case report
- PMID: 38006608
- PMCID: PMC10683565
- DOI: 10.1177/03000605231213751
Pediatric headache patient with cerebral abscesses: a brief review of the literature and case report
Abstract
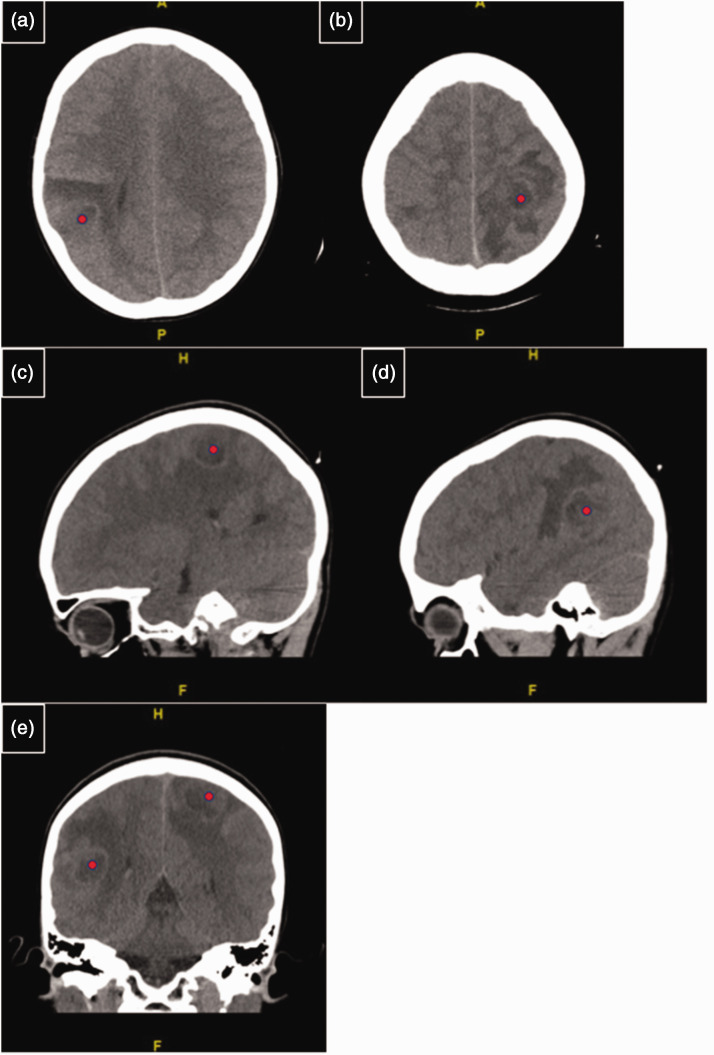
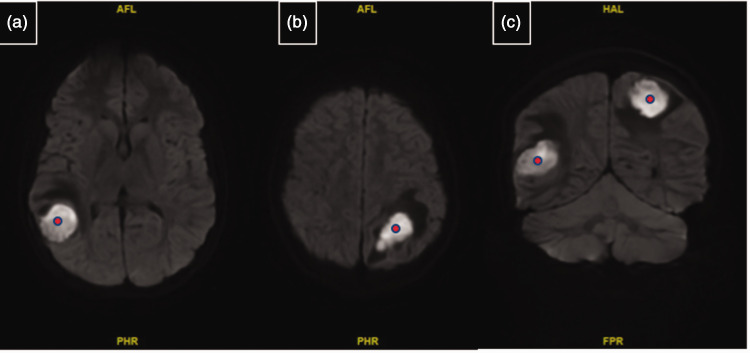
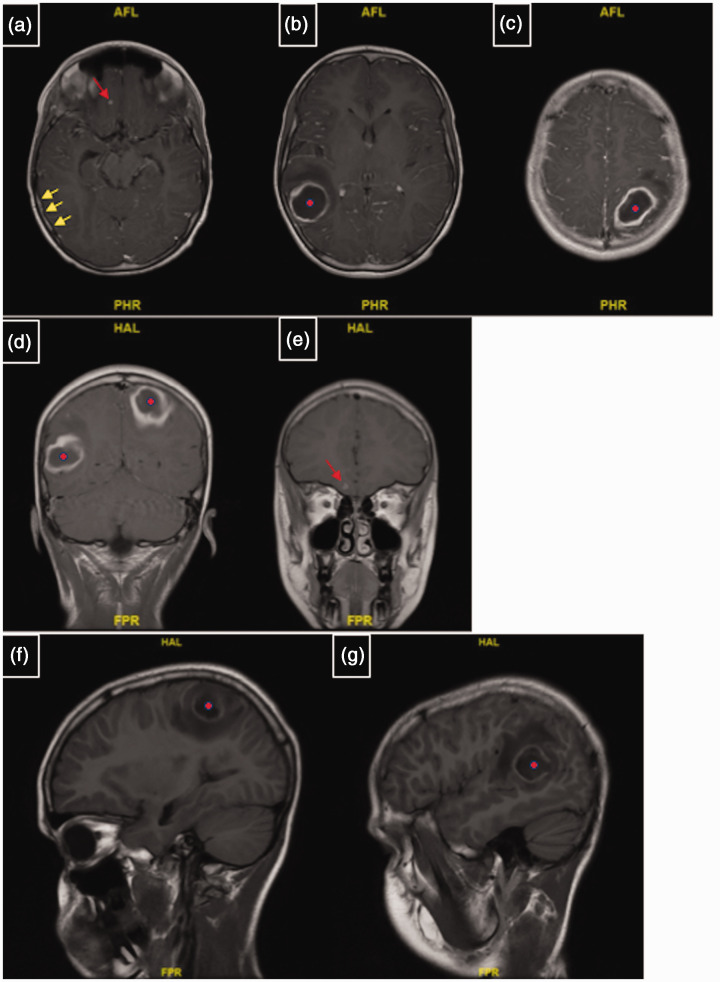
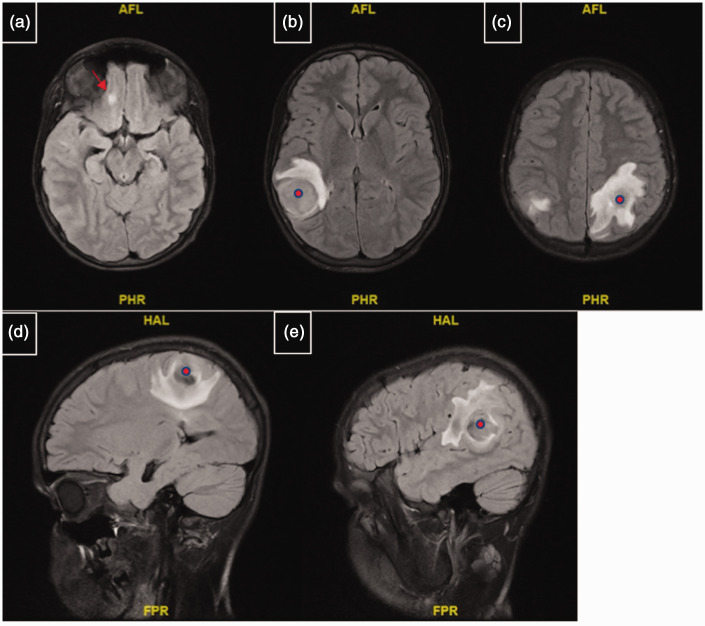
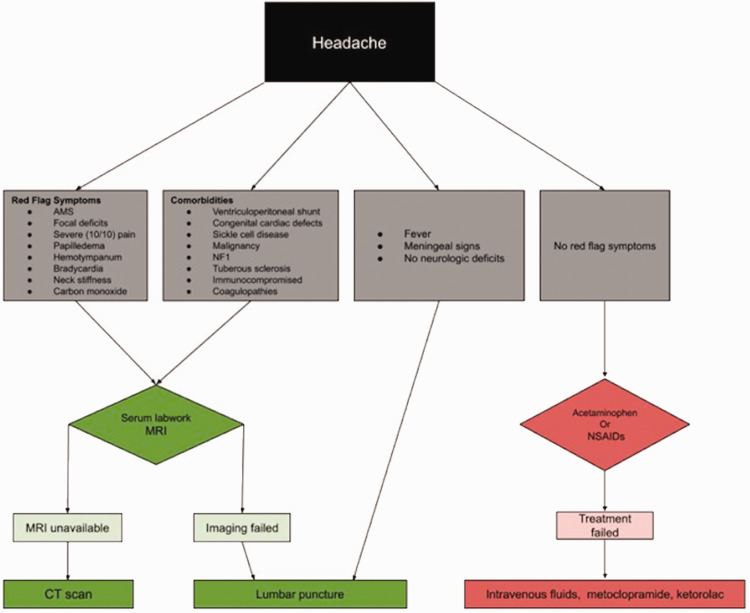
Background: Pediatric headache is a common cause of pediatric emergency department (ED) visits, and 8.8% of cases require imaging. Alarmingly, 12.5% of imaged cases have a pathologic cause. A pediatric patient with a complicated medical history presented to the pediatric ED with multiple cerebral abscesses. The possible causes and contributors to this rare cause of pediatric headache and a review of pediatric headache emergency management are presented.Case Presentation: A 12-year-old male patient with a complex medical and surgical history, including post-repair pulmonary valve stenosis, visited the pediatric ED for intractable and worsening left frontoparietal headache, refractory to ibuprofen, for 6 days. A physical examination revealed severe photophobia and restlessness secondary to severe head pain. Non-contrast brain computed tomography demonstrated two round, bilateral, parietal hypodense lesions with surrounding vasogenic edema. The lesions were consistent with abscesses on magnetic resonance imaging. Eventually, the patient underwent successful surgical abscess drainage and made a full recovery. The patient was lost to follow-up; therefore, no causative bacterial species was determined.
Conclusion: Managing pediatric headache in emergency settings requires a robust history and physical examination. Cerebral abscesses are an infrequent but fatal cause of pediatric headache and therefore should be considered among the differential diagnoses.
Keywords: Cerebral abscess; brain imaging; case report; congenital defect; pediatric brain lesion; pediatric headache.
Conflict of interest statement
Declaration of conflicting interestsThe authors declare that there is no conflict of interest.
Figures
Similar articles
-
Tuberculous brain abscess in a patient with AIDS: case report and literature review.Rev Inst Med Trop Sao Paulo. 2003 Mar-Apr;45(2):111-4. doi: 10.1590/s0036-46652003000200013. Epub 2003 May 14. Rev Inst Med Trop Sao Paulo. 2003. PMID: 12754580 Review.
-
A rare case of brain abscess caused by Actinomyces meyeri.BMC Infect Dis. 2020 May 27;20(1):378. doi: 10.1186/s12879-020-05100-9. BMC Infect Dis. 2020. PMID: 32460724 Free PMC article.
-
[A man in his thirties with recurrent brain abscesses].Tidsskr Nor Laegeforen. 2022 Dec 12;142(18). doi: 10.4045/tidsskr.21.0811. Print 2022 Dec 13. Tidsskr Nor Laegeforen. 2022. PMID: 36511743 Norwegian.
-
An 11-year-old girl with right-sided weakness secondary to cerebral abscesses: a case report.Pediatr Emerg Care. 2013 Mar;29(3):360-3. doi: 10.1097/PEC.0b013e3182854645. Pediatr Emerg Care. 2013. PMID: 23462391
-
Primary pituitary abscess in an adolescent female patient: case report, literature review, and operative video.Childs Nerv Syst. 2021 May;37(5):1423-1428. doi: 10.1007/s00381-021-05052-8. Epub 2021 Jan 29. Childs Nerv Syst. 2021. PMID: 33515057 Review.
References
-
- Gagnier JJ, Kienle G, Altman DG, et al.. The CARE guidelines: consensus-based clinical case reporting guideline development. Headache 2013; 53: 1541–1547. DOI: 10.1111/head.12246. - PubMed
-
- Robbins MS, Lipton RB. The epidemiology of primary headache disorders. Semin Neurol 2010; 30: 107–119. DOI: 10.1055/s-0030-1249220. - PubMed
-
- Lateef TM, Grewal M, McClintock W, et al.. Headache in young children in the emergency department: use of computed tomography. Pediatrics 2009; 124: E12–E17. DOI: 10.1542/peds.2008-3150. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
