

Salivary IgA and vimentin differentiate in vitro SARS-CoV-2 infection: A study of 290 convalescent COVID-19 patients
- PMID: 38007005
- PMCID: PMC11139657
- DOI: 10.1016/j.mucimm.2023.11.007
Salivary IgA and vimentin differentiate in vitro SARS-CoV-2 infection: A study of 290 convalescent COVID-19 patients
Abstract
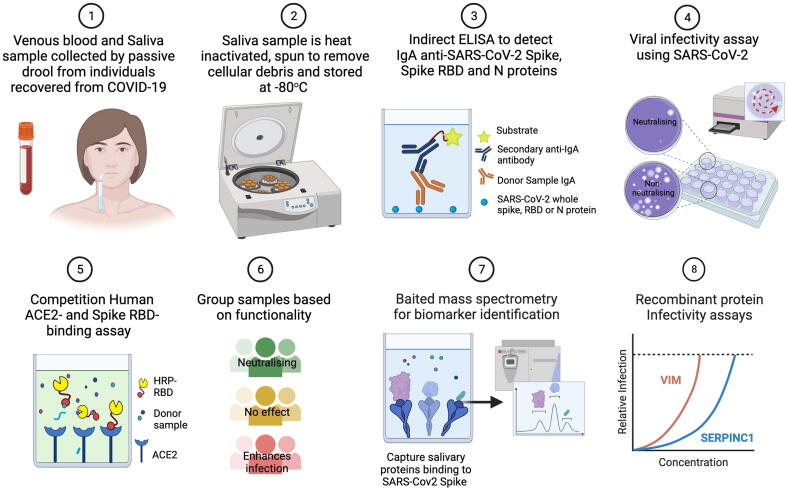
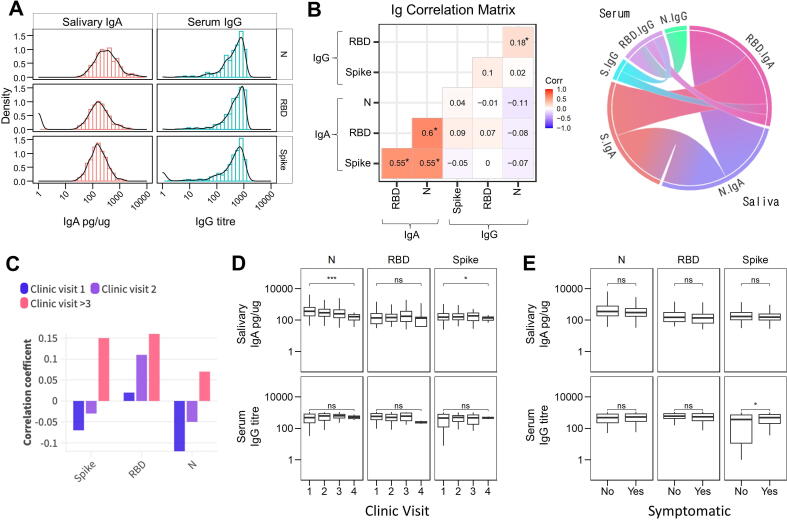
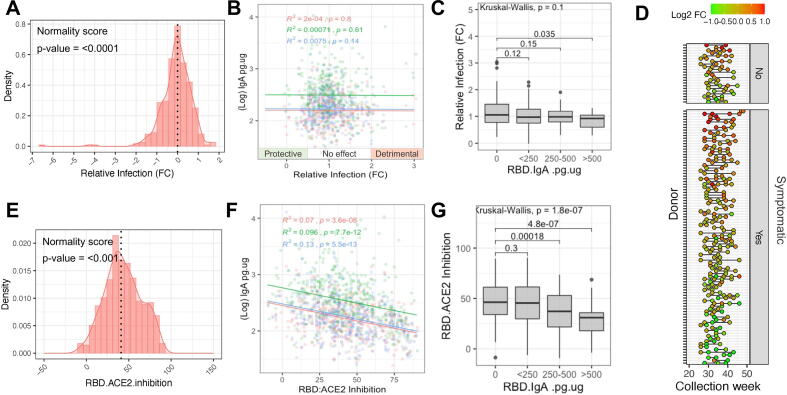
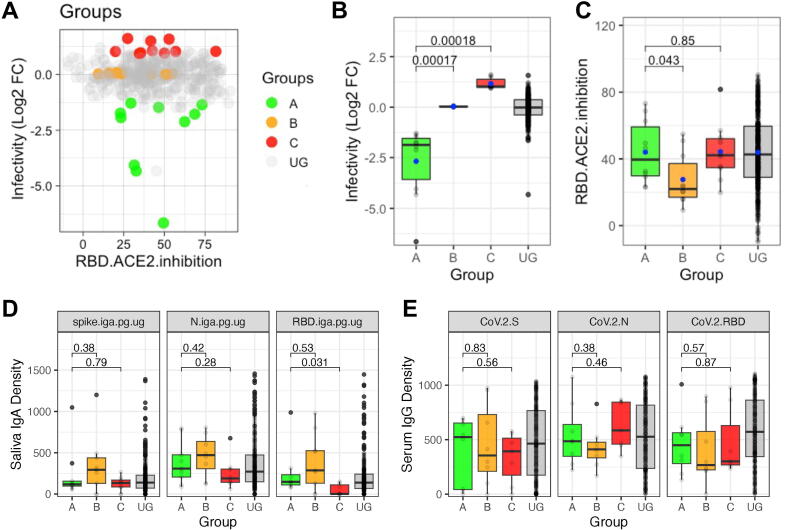
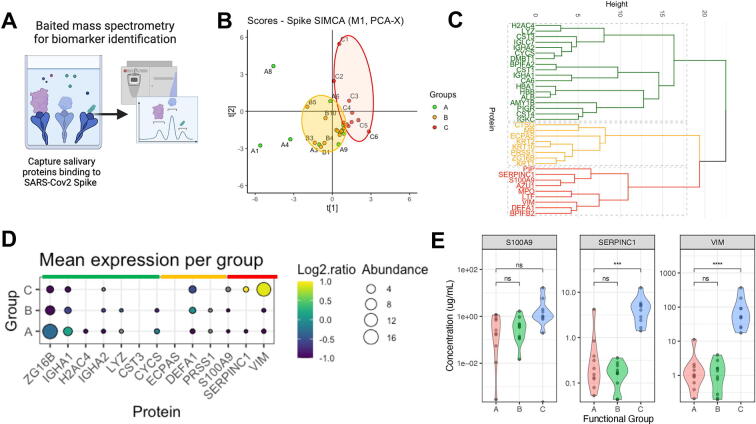
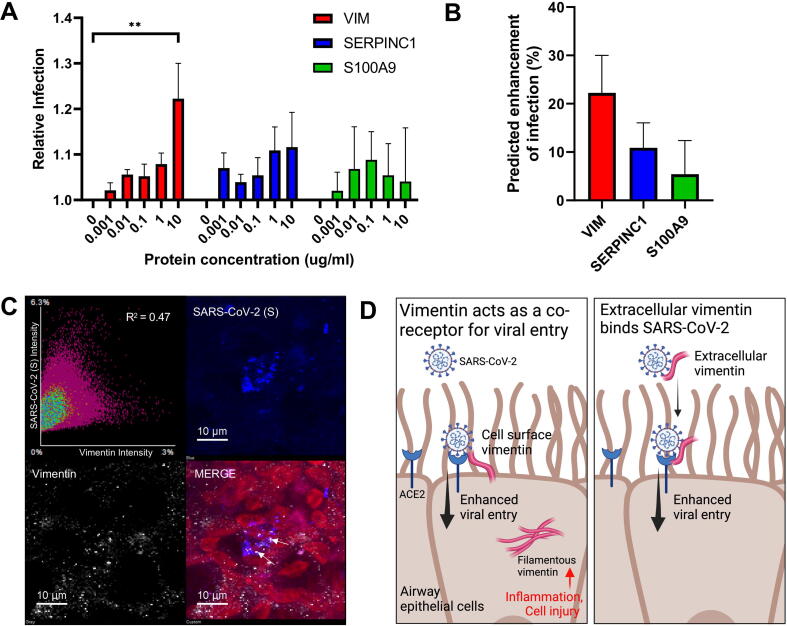
SARS-CoV-2 initially infects cells in the nasopharynx and oral cavity. The immune system at these mucosal sites plays a crucial role in minimizing viral transmission and infection. To develop new strategies for preventing SARS-CoV-2 infection, this study aimed to identify proteins that protect against viral infection in saliva. We collected 551 saliva samples from 290 healthcare workers who had tested positive for COVID-19, before vaccination, between June and December 2020. The samples were categorized based on their ability to block or enhance infection using in vitro assays. Mass spectrometry and enzyme-linked immunosorbent assay experiments were used to identify and measure the abundance of proteins that specifically bind to SARS-CoV-2 antigens. Immunoglobulin (Ig)A specific to SARS-CoV-2 antigens was detectable in over 83% of the convalescent saliva samples. We found that concentrations of anti-receptor-binding domain IgA >500 pg/µg total protein in saliva correlate with reduced viral infectivity in vitro. However, there is a dissociation between the salivary IgA response to SARS-CoV-2, and systemic IgG titers in convalescent COVID-19 patients. Then, using an innovative technique known as spike-baited mass spectrometry, we identified novel spike-binding proteins in saliva, most notably vimentin, which correlated with increased viral infectivity in vitro and could serve as a therapeutic target against COVID-19.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Salivary and serum IgA and IgG responses to SARS-CoV-2-spike protein following SARS-CoV-2 infection and after immunization with COVID-19 vaccines.Allergy Asthma Proc. 2022 Sep 1;43(5):419-430. doi: 10.2500/aap.2022.43.220045. Allergy Asthma Proc. 2022. PMID: 36065108 Free PMC article.
-
Persistence of serum and saliva antibody responses to SARS-CoV-2 spike antigens in COVID-19 patients.Sci Immunol. 2020 Oct 8;5(52):eabe5511. doi: 10.1126/sciimmunol.abe5511. Sci Immunol. 2020. PMID: 33033173 Free PMC article.
-
Development and Validation of an Enzyme Immunoassay for Detection and Quantification of SARS-CoV-2 Salivary IgA and IgG.J Immunol. 2022 Mar 15;208(6):1500-1508. doi: 10.4049/jimmunol.2100934. Epub 2022 Feb 28. J Immunol. 2022. PMID: 35228262 Free PMC article.
-
Systemic and mucosal IgA responses are variably induced in response to SARS-CoV-2 mRNA vaccination and are associated with protection against subsequent infection.Mucosal Immunol. 2022 May;15(5):799-808. doi: 10.1038/s41385-022-00511-0. Epub 2022 Apr 25. Mucosal Immunol. 2022. PMID: 35468942 Free PMC article.
-
Saliva is suitable for SARS-CoV-2 antibodies detection after vaccination: A rapid systematic review.Front Immunol. 2022 Sep 20;13:1006040. doi: 10.3389/fimmu.2022.1006040. eCollection 2022. Front Immunol. 2022. PMID: 36203571 Free PMC article.
Cited by
-
COVID-19 mRNA Vaccines Induce Robust Levels of IgG but Limited Amounts of IgA Within the Oronasopharynx of Young Children.J Infect Dis. 2024 Dec 16;230(6):1390-1399. doi: 10.1093/infdis/jiae450. J Infect Dis. 2024. PMID: 39253950
-
COVID-19 mRNA vaccines induce robust levels of IgG but limited amounts of IgA within the oronasopharynx of young children.medRxiv [Preprint]. 2024 Apr 16:2024.04.15.24305767. doi: 10.1101/2024.04.15.24305767. medRxiv. 2024. Update in: J Infect Dis. 2024 Dec 16;230(6):1390-1399. doi: 10.1093/infdis/jiae450. PMID: 38699375 Free PMC article. Updated. Preprint.
-
Extracellular vimentin is a damage-associated molecular pattern protein serving as an agonist of TLR4 in human neutrophils.Cell Commun Signal. 2025 Feb 5;23(1):64. doi: 10.1186/s12964-025-02062-w. Cell Commun Signal. 2025. PMID: 39910535 Free PMC article.
References
-
- Asahi-Ozaki Y., et al. Secretory IgA antibodies provide cross-protection against infection with different strains of influenza B virus. J. Med. Virol. 2004;74:328–335. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
