

Multi-site microbiota alteration is a hallmark of kidney stone formation
- PMID: 38007438
- PMCID: PMC10675928
- DOI: 10.1186/s40168-023-01703-x
Multi-site microbiota alteration is a hallmark of kidney stone formation
Abstract
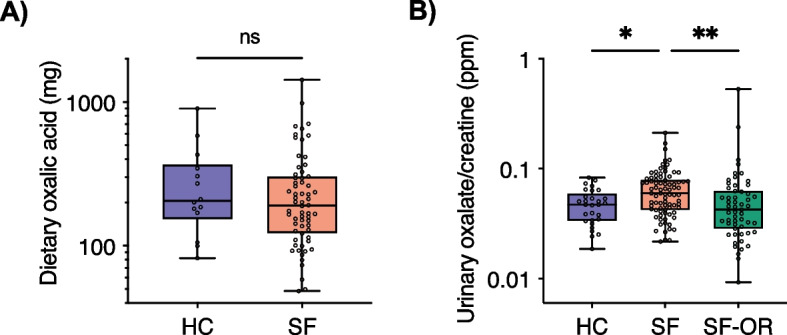
Background: Inquiry of microbiota involvement in kidney stone disease (KSD) has largely focussed on potential oxalate handling abilities by gut bacteria and the increased association with antibiotic exposure. By systematically comparing the gut, urinary, and oral microbiota of 83 stone formers (SF) and 30 healthy controls (HC), we provide a unified assessment of the bacterial contribution to KSD.
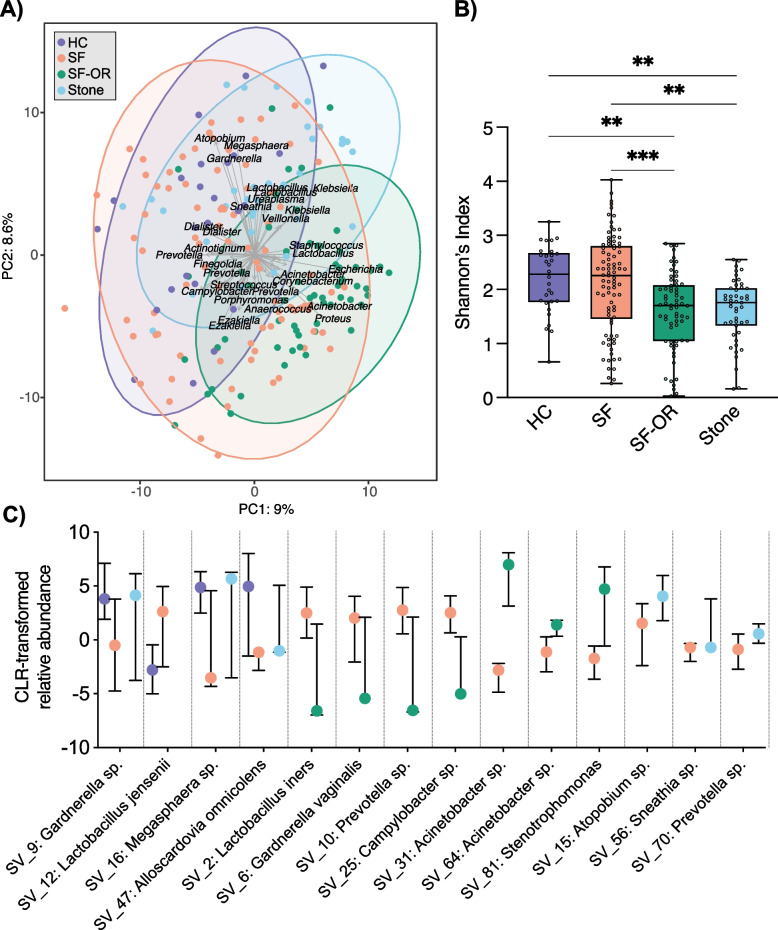
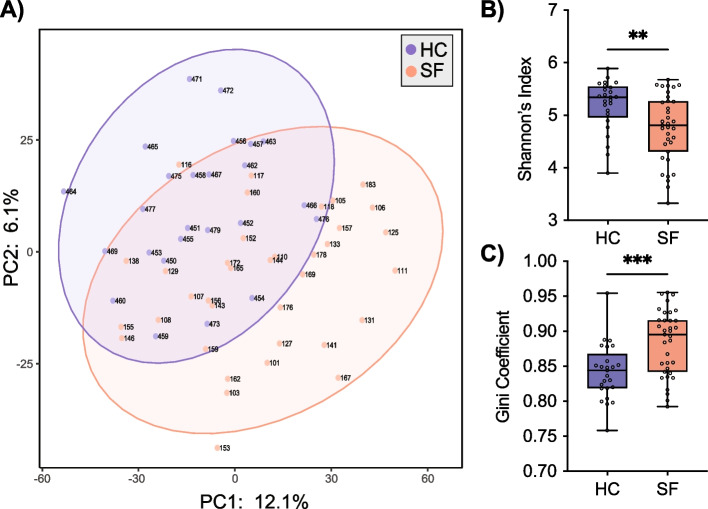
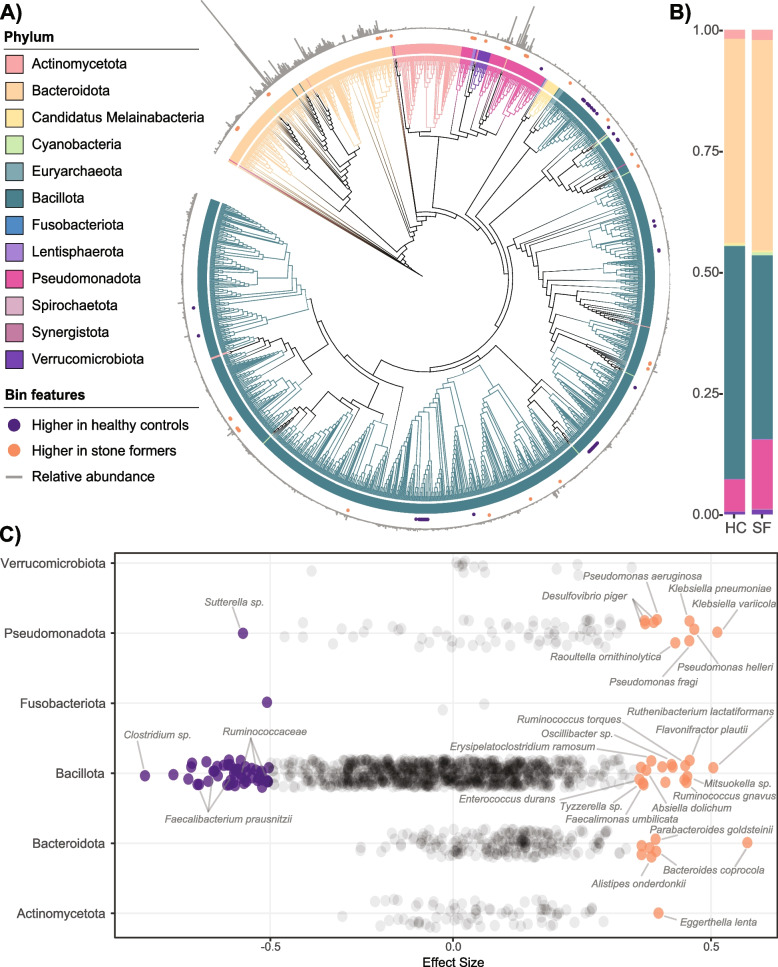
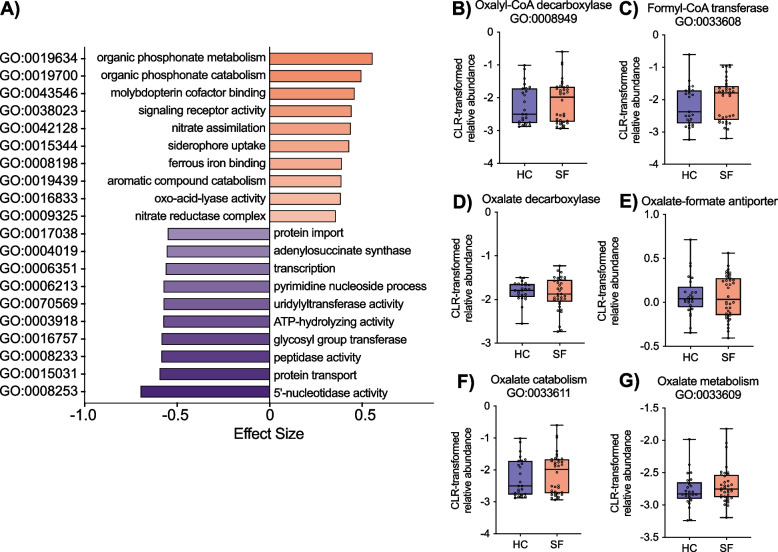
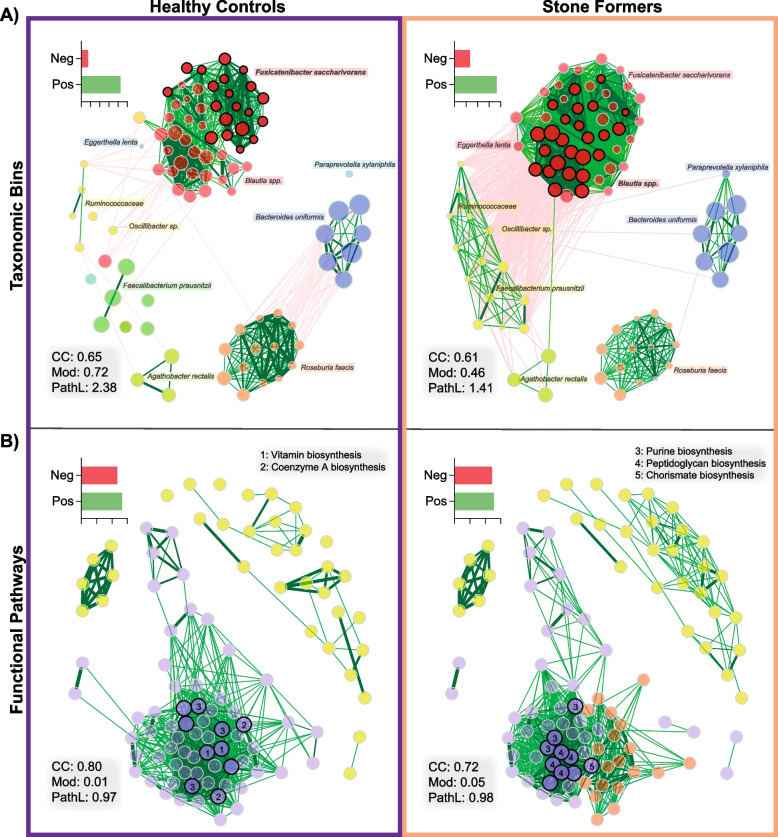
Results: Amplicon and shotgun metagenomic sequencing approaches were consistent in identifying multi-site microbiota disturbances in SF relative to HC. Biomarker taxa, reduced taxonomic and functional diversity, functional replacement of core bioenergetic pathways with virulence-associated gene markers, and community network collapse defined SF, but differences between cohorts did not extend to oxalate metabolism.
Conclusions: We conclude that multi-site microbiota alteration is a hallmark of SF, and KSD treatment should consider microbial functional restoration and the avoidance of aberrant modulators such as poor diet and antibiotics where applicable to prevent stone recurrence. Video Abstract.
Keywords: Gut microbiota; Kidney stones; Microbiota; Shotgun metagenomic sequencing; Urinary microbiota; Urology.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Abufaraj M, Xu T, Cao C, Waldhoer T, Seitz C, D'Andrea D, Siyam A, Tarawneh R, Fajkovic H, Schernhammer E, et al. Prevalence and Trends in Kidney Stone Among Adults in the USA: Analyses of National Health and Nutrition Examination Survey 2007–2018 Data. Eur Urol Focus. 2021;7:1468–1475. doi: 10.1016/j.euf.2020.08.011. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
