

Non-alcoholic fatty liver disease risk prediction model and health management strategies for older Chinese adults: a cross-sectional study
- PMID: 38007441
- PMCID: PMC10675849
- DOI: 10.1186/s12944-023-01966-1
Non-alcoholic fatty liver disease risk prediction model and health management strategies for older Chinese adults: a cross-sectional study
Abstract
Background: Non-alcoholic fatty liver disease (NAFLD) is a common chronic liver condition that affects a quarter of the global adult population. To date, only a few NAFLD risk prediction models have been developed for Chinese older adults aged ≥ 60 years. This study presented the development of a risk prediction model for NAFLD in Chinese individuals aged ≥ 60 years and proposed personalised health interventions based on key risk factors to reduce NAFLD incidence among the population.
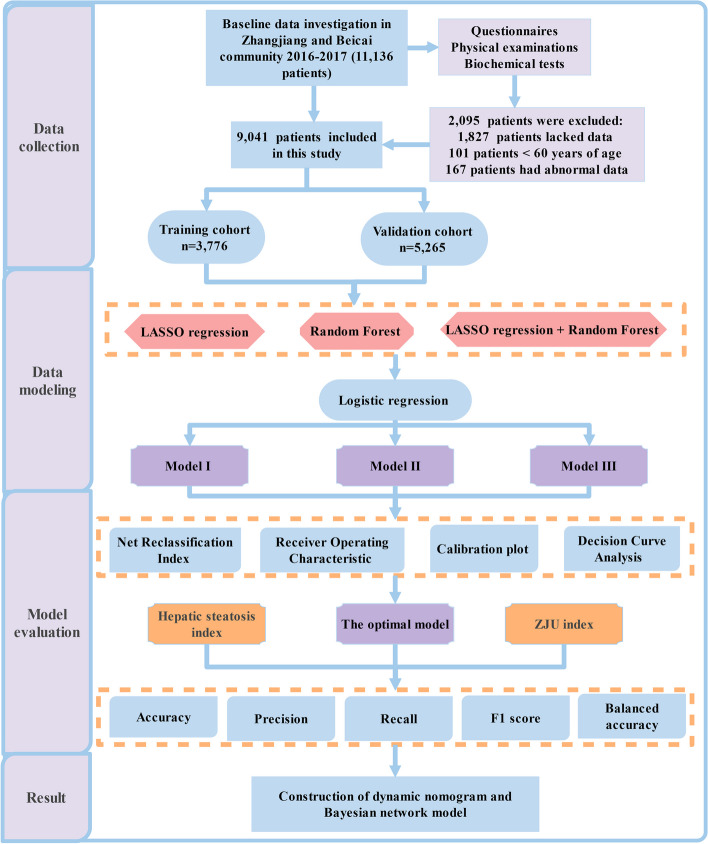
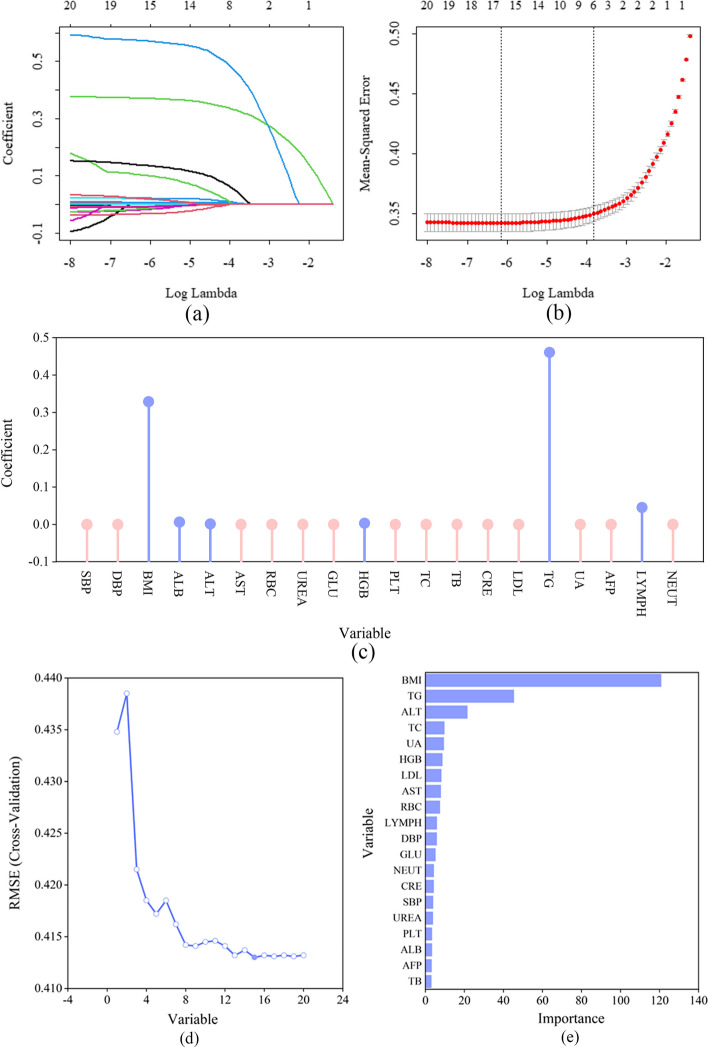
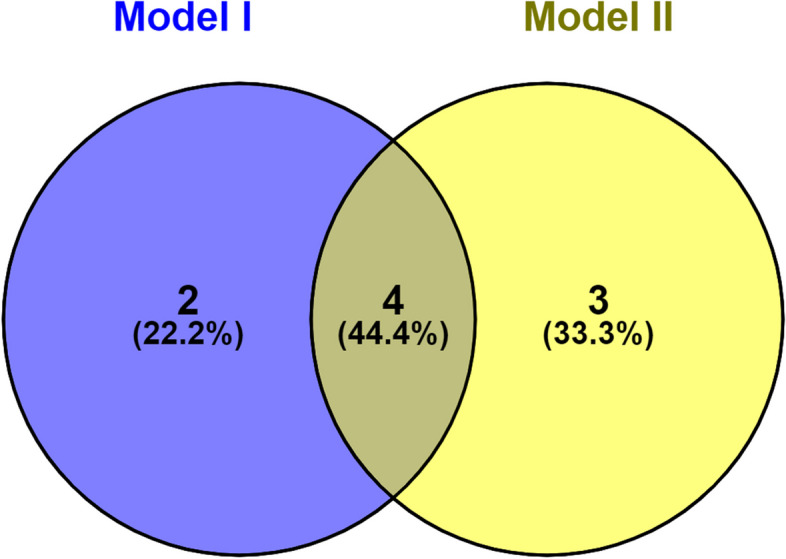
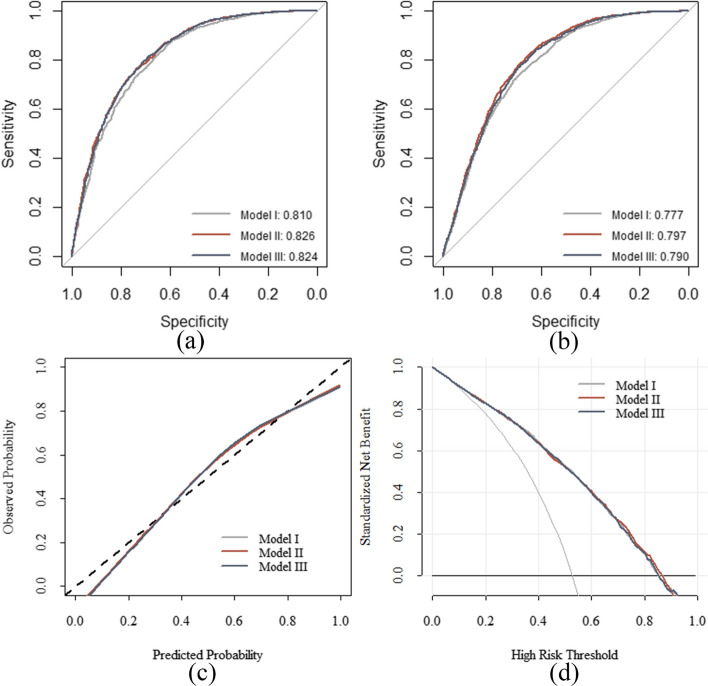
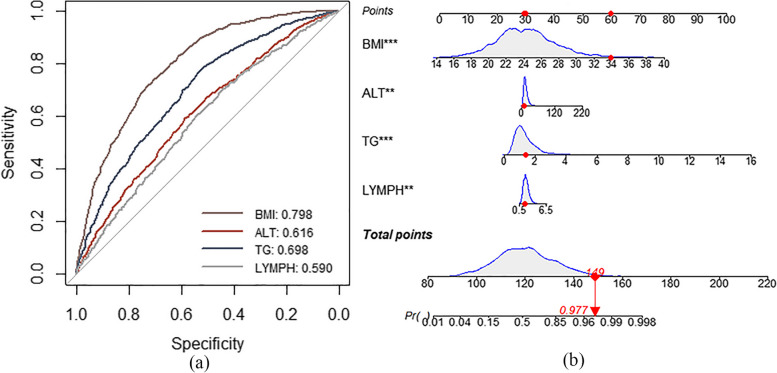
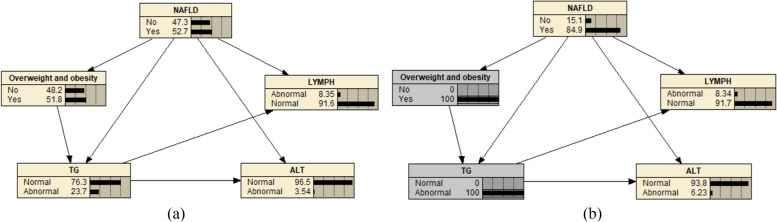
Methods: A cross-sectional survey was carried out among 9,041 community residents in Shanghai. Three NAFLD risk prediction models (I, II, and III) were constructed using multivariate logistic regression analysis based on the least absolute shrinkage and selection operator regression analysis, and random forest model to select individual characteristics, respectively. To determine the optimal model, the three models' discrimination, calibration, clinical application, and prediction capability were evaluated using the receiver operating characteristic (ROC) curve, calibration plot, decision curve analysis, and net reclassification index (NRI), respectively. To evaluate the optimal model's effectiveness, the previously published NAFLD risk prediction models (Hepatic steatosis index [HSI] and ZJU index) were evaluated using the following five indicators: accuracy, precision, recall, F1-score, and balanced accuracy. A dynamic nomogram was constructed for the optimal model, and a Bayesian network model for predicting NAFLD risk in older adults was visually displayed using Netica software.
Results: The area under the ROC curve of Models I, II, and III in the training dataset was 0.810, 0.826, and 0.825, respectively, and that of the testing data was 0.777, 0.797, and 0.790, respectively. No significant difference was found in the accuracy or NRI between the models; therefore, Model III with the fewest variables was determined as the optimal model. Compared with the HSI and ZJU index, Model III had the highest accuracy (0.716), precision (0.808), recall (0.605), F1 score (0.692), and balanced accuracy (0.723). The risk threshold for Model III was 20%-80%. Model III included body mass index, alanine aminotransferase level, triglyceride level, and lymphocyte count.
Conclusions: A dynamic nomogram and Bayesian network model were developed to identify NAFLD risk in older Chinese adults, providing personalized health management strategies and reducing NAFLD incidence.
Keywords: Bayesian network; Chinese older adults; Health management strategies; Nomogram; Non-alcoholic fatty liver disease.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Cotter TG, Rinella M. Nonalcoholic Fatty Liver Disease 2020: The State of the Disease. Gastroenterology. 2020;158:1851–1864. - PubMed
-
- Makri E, Goulas A, Polyzos SA. Epidemiology, pathogenesis, diagnosis and emerging treatment of nonalcoholic fatty liver disease. Arch Med Res. 2021;52:25–37. - PubMed
-
- Riazi K, Azhari H, Charette JH, Underwood FE, King JA, Afshar EE, Swain MG, Congly SE, Kaplan GG, Shaheen AA. The prevalence and incidence of NAFLD worldwide: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2022;7:851–861. - PubMed
-
- Li J, Zou B, Yeo YH, Feng Y, Xie X, Lee DH, Fujii H, Wu Y, Kam LY, Ji F, et al. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999–2019: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2019;4:389–398. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
