

Multi-omics analysis of hospital-acquired diarrhoeal patients reveals biomarkers of enterococcal proliferation and Clostridioides difficile infection
- PMID: 38007555
- PMCID: PMC10676382
- DOI: 10.1038/s41467-023-43671-8
Multi-omics analysis of hospital-acquired diarrhoeal patients reveals biomarkers of enterococcal proliferation and Clostridioides difficile infection
Abstract
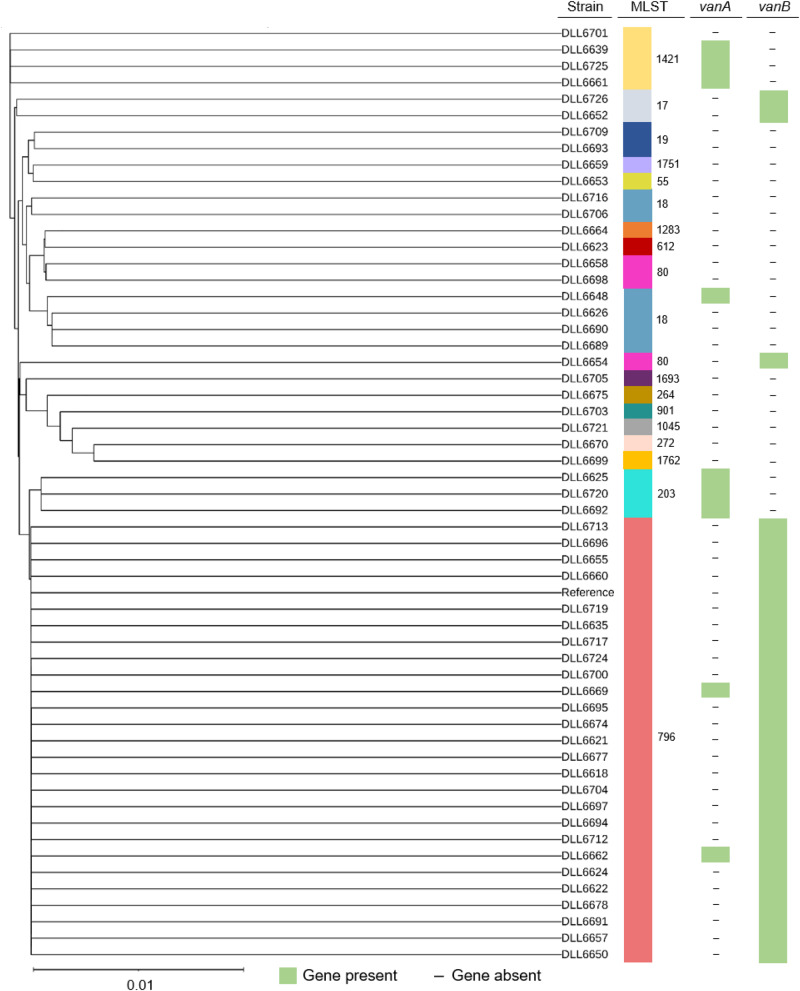
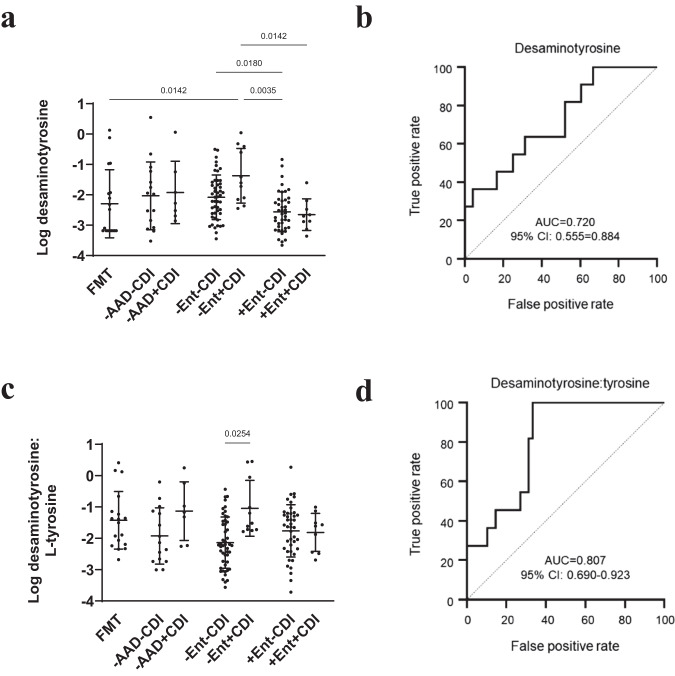
Hospital-acquired diarrhoea (HAD) is common, and often associated with gut microbiota and metabolome dysbiosis following antibiotic administration. Clostridioides difficile is the most significant antibiotic-associated diarrhoeal (AAD) pathogen, but less is known about the microbiota and metabolome associated with AAD and C. difficile infection (CDI) with contrasting antibiotic treatment. We characterised faecal microbiota and metabolome for 169 HAD patients (33 with CDI and 133 non-CDI) to determine dysbiosis biomarkers and gain insights into metabolic strategies C. difficile might use for gut colonisation. The specimen microbial community was analysed using 16 S rRNA gene amplicon sequencing, coupled with untargeted metabolite profiling using gas chromatography-mass spectrometry (GC-MS), and short-chain fatty acid (SCFA) profiling using GC-MS. AAD and CDI patients were associated with a spectrum of dysbiosis reflecting non-antibiotic, short-term, and extended-antibiotic treatment. Notably, extended antibiotic treatment was associated with enterococcal proliferation (mostly vancomycin-resistant Enterococcus faecium) coupled with putative biomarkers of enterococcal tyrosine decarboxylation. We also uncovered unrecognised metabolome dynamics associated with concomitant enterococcal proliferation and CDI, including biomarkers of Stickland fermentation and amino acid competition that could distinguish CDI from non-CDI patients. Here we show, candidate metabolic biomarkers for diagnostic development with possible implications for CDI and vancomycin-resistant enterococci (VRE) treatment.
© 2023. Crown.
Conflict of interest statement
The authors declare no competing interests.
Figures






Similar articles
-
Gut metabolites predict Clostridioides difficile recurrence.Microbiome. 2022 Jun 9;10(1):87. doi: 10.1186/s40168-022-01284-1. Microbiome. 2022. PMID: 35681218 Free PMC article.
-
Dysbiosis of the gut microbiota is associated with in-hospital mortality in patients with antibiotic-associated diarrhoea: A metagenomic analysis.Int J Antimicrob Agents. 2024 Nov;64(5):107330. doi: 10.1016/j.ijantimicag.2024.107330. Epub 2024 Sep 6. Int J Antimicrob Agents. 2024. PMID: 39244165
-
Microbiota-based markers predictive of development of Clostridioides difficile infection.Nat Commun. 2021 Apr 14;12(1):2241. doi: 10.1038/s41467-021-22302-0. Nat Commun. 2021. PMID: 33854066 Free PMC article.
-
The role of the gut microbiome in colonization resistance and recurrent Clostridioides difficile infection.Therap Adv Gastroenterol. 2022 Nov 18;15:17562848221134396. doi: 10.1177/17562848221134396. eCollection 2022. Therap Adv Gastroenterol. 2022. PMID: 36425405 Free PMC article. Review.
-
Ridinilazole: a novel, narrow-spectrum antimicrobial agent targeting Clostridium (Clostridioides) difficile.Lett Appl Microbiol. 2022 Sep;75(3):526-536. doi: 10.1111/lam.13664. Epub 2022 Feb 11. Lett Appl Microbiol. 2022. PMID: 35119124 Free PMC article. Review.
Cited by
-
Polysaccharides of natural products alleviate antibiotic-associated diarrhea by regulating gut microbiota: a review.Arch Microbiol. 2024 Nov 7;206(12):461. doi: 10.1007/s00203-024-04184-0. Arch Microbiol. 2024. PMID: 39508892 Review.
-
Phage lysins for intestinal microbiome modulation: current challenges and enabling techniques.Gut Microbes. 2024 Jan-Dec;16(1):2387144. doi: 10.1080/19490976.2024.2387144. Epub 2024 Aug 6. Gut Microbes. 2024. PMID: 39106212 Free PMC article. Review.
-
Prioritizing isolation precautions: a patient-centered approach to infection prevention and control.Antimicrob Steward Healthc Epidemiol. 2025 Jun 3;5(1):e123. doi: 10.1017/ash.2025.173. eCollection 2025. Antimicrob Steward Healthc Epidemiol. 2025. PMID: 40528936 Free PMC article. Review.
-
Protection against Clostridioides difficile disease by a naturally avirulent strain.Cell Host Microbe. 2025 Jan 8;33(1):59-70.e4. doi: 10.1016/j.chom.2024.11.003. Epub 2024 Nov 27. Cell Host Microbe. 2025. PMID: 39610252
-
Biotransformation of Canola Feedstock Waste Using Brassica Pest Microbiome: Proof of Concept for Insects as Bioengineers.Int J Mol Sci. 2025 Aug 9;26(16):7715. doi: 10.3390/ijms26167715. Int J Mol Sci. 2025. PMID: 40869039 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Miscellaneous
