

Preoperative Rehabilitation Is Feasible in the Weeks Prior to Surgery and Significantly Improves Functional Performance
- PMID: 38008976
- PMCID: PMC10683858
- DOI: 10.14283/jfa.2022.42
Preoperative Rehabilitation Is Feasible in the Weeks Prior to Surgery and Significantly Improves Functional Performance
Abstract
Background: Frailty is a multidimensional state of increased vulnerability. Frail patients are at increased risk for poor surgical outcomes. Prior research demonstrates that rehabilitation strategies deployed after surgery improve outcomes by building strength.
Objectives: Examine the feasibility and impact of a novel, multi-faceted prehabilitation intervention for frail patients before surgery.
Design: Single arm clinical trial.
Setting: Veterans Affairs hospital.
Participants: Patients preparing for major abdominal, urological, thoracic, or cardiac surgery with frailty identified as a Risk Analysis Index≥30.
Intervention: Prehabilitation started in a supervised setting to establish safety and then transitioned to home-based exercise with weekly telephone coaching by exercise physiologists. Prehabilitation included (a)strength and coordination training; (b)respiratory muscle training (IMT); (c)aerobic conditioning; and (d)nutritional coaching and supplementation. Prehabilitation length was tailored to the 4-6 week time lag typically preceding each participant's normally scheduled surgery.
Measurements: Functional performance and patient surveys were assessed at baseline, every other week during prehabilitation, and then 30 and 90 days after surgery. Within-person changes were estimated using linear mixed models.
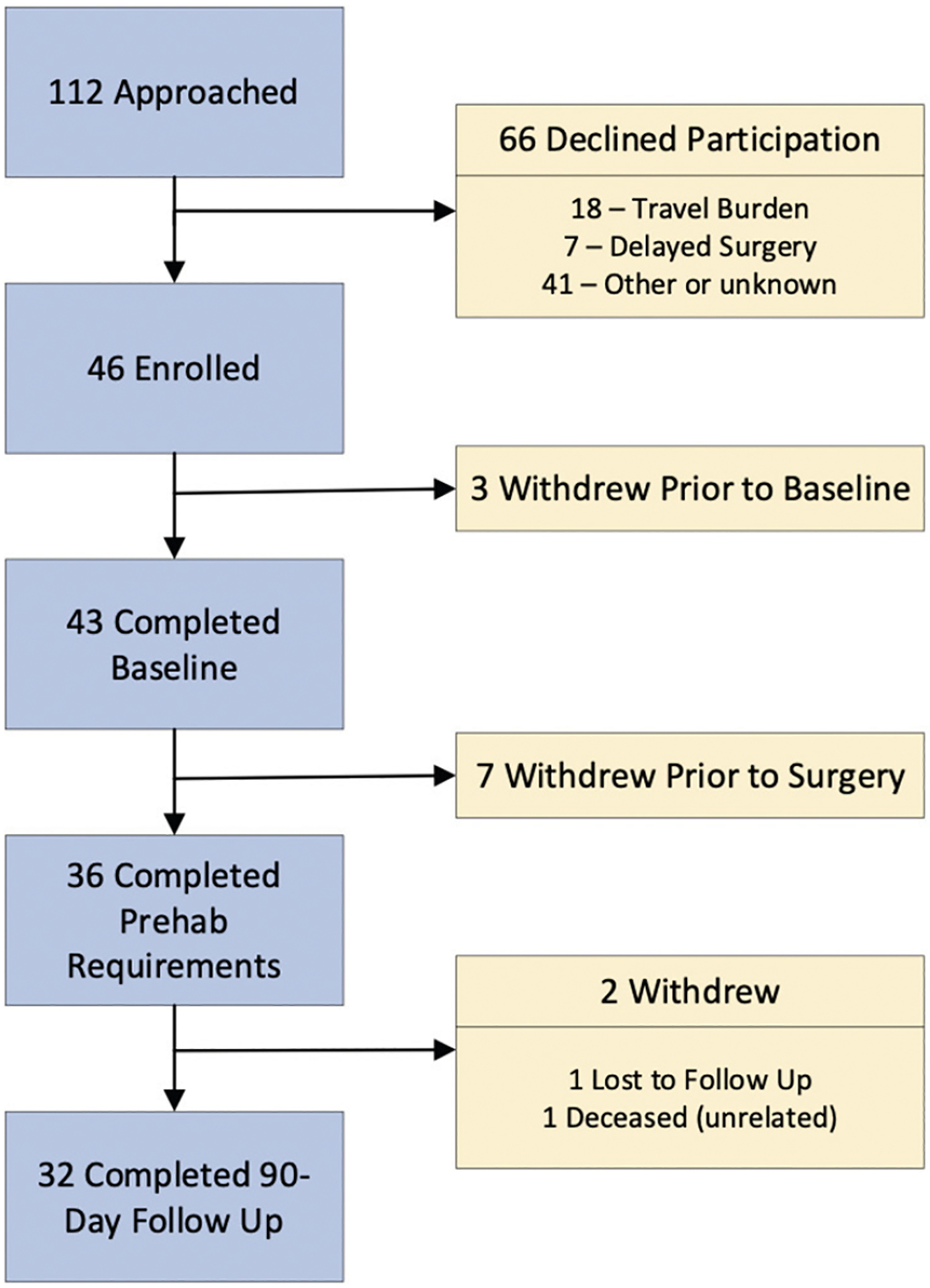
Results: 43 patients completed baseline assessments; 36(84%) completed a median 5(range 3-10) weeks of prehabilitation before surgery; 32(74%) were retained through 90-day follow-up. Baseline function was relatively low. Exercise logs show participants completed 94% of supervised exercise, 78% of prescribed IMT and 74% of home-based exercise. Between baseline and day of surgery, timed-up-and-go decreased 2.3 seconds, gait speed increased 0.1 meters/second, six-minute walk test increased 41.7 meters, and the time to complete 5 chair rises decreased 1.6 seconds(all P≤0.007). Maximum and mean inspiratory and expiratory pressures increased 4.5, 7.3, 14.1 and 13.5 centimeters of water, respectively(all P≤0.041).
Conclusions: Prehabilitation is feasible before major surgery and achieves clinically meaningful improvements in functional performance that may impact postoperative outcomes and recovery. These data support rationale for a larger trial powered to detect differences in postoperative outcomes.
Keywords: Frailty; prehabilitation; rehabilitation; surgery.
Conflict of interest statement
Portions of these data were presented at the 2021 ICFSR (virtual) on September 29, 2021. Dr. Hall reports a consulting relationship with FutureAssure, LLC. Dr. Wilson reports grants from Veterans Affairs Office of Research and Development during the conduct of the study. Authors Youk, Allsup, Kennedy, Byard, Dhupar, Chu, Rahman, Cahalin, Afilalo, and Forman declare no conflict of interest.
Figures
Similar articles
-
Recovery of surgery in the elderly (ROSE) program: The efficacy of a multi-modal prehabilitation program implemented in frail and pre-frail elderly undergoing major abdominal surgery.World J Surg. 2024 Jan;48(1):48-58. doi: 10.1002/wjs.12016. Epub 2023 Dec 15. World J Surg. 2024. PMID: 38686802
-
Home-based prehabilitation with exercise to improve postoperative recovery for older adults with frailty having cancer surgery: the PREHAB randomised clinical trial.Br J Anaesth. 2022 Jul;129(1):41-48. doi: 10.1016/j.bja.2022.04.006. Epub 2022 May 17. Br J Anaesth. 2022. PMID: 35589429 Clinical Trial.
-
Barriers and facilitators to participation in exercise prehabilitation before cancer surgery for older adults with frailty: a qualitative study.BMC Geriatr. 2023 Jun 6;23(1):356. doi: 10.1186/s12877-023-03990-3. BMC Geriatr. 2023. PMID: 37280523 Free PMC article. Clinical Trial.
-
The role of prehabilitation in frail surgical patients: A systematic review.Acta Anaesthesiol Scand. 2018 Nov;62(10):1356-1366. doi: 10.1111/aas.13239. Epub 2018 Aug 10. Acta Anaesthesiol Scand. 2018. PMID: 30094821
-
Concepts for exercise therapy in prehabilitation for elderly people with frailty or pre-frailty prior to elective surgery. A scoping review.J Bodyw Mov Ther. 2023 Oct;36:74-82. doi: 10.1016/j.jbmt.2023.05.004. Epub 2023 Jun 12. J Bodyw Mov Ther. 2023. PMID: 37949603
Cited by
-
Various Forms of Cardiac Rehabilitation and Their Effect on Frailty Syndrome in Cardiac Patients-A Systematic Review.Healthcare (Basel). 2024 Nov 29;12(23):2401. doi: 10.3390/healthcare12232401. Healthcare (Basel). 2024. PMID: 39685023 Free PMC article. Review.
-
Decision making in the frail vascular surgery patient: A scoping review.Semin Vasc Surg. 2024 Jun;37(2):224-239. doi: 10.1053/j.semvascsurg.2024.04.003. Epub 2024 Apr 21. Semin Vasc Surg. 2024. PMID: 39152001 Free PMC article.
-
The Surgical Pause: The Importance of Measuring Frailty and Taking Action to Address Identified Frailty.Jt Comm J Qual Patient Saf. 2025 Mar;51(3):167-177. doi: 10.1016/j.jcjq.2024.11.011. Epub 2024 Nov 22. Jt Comm J Qual Patient Saf. 2025. PMID: 39799070
-
Inspiratory Muscle and Functional Performance of Patients Entering Cardiac Rehabilitation after Cardiac Valve Replacement.J Cardiovasc Dev Dis. 2023 Mar 28;10(4):142. doi: 10.3390/jcdd10040142. J Cardiovasc Dev Dis. 2023. PMID: 37103021 Free PMC article.
-
Feasibility of preoperative and postoperative physical rehabilitation for cardiac surgery patients - a longitudinal cohort study.BMC Sports Sci Med Rehabil. 2023 Dec 19;15(1):173. doi: 10.1186/s13102-023-00786-1. BMC Sports Sci Med Rehabil. 2023. PMID: 38115103 Free PMC article.
References
-
- McDermid RC, Bagshaw SM. Physiological Reserve and Frailty in Critical Illness. In: Textbook of Post-ICU Medicine: The Legacy of Critical Care. Oxford, UK: Oxford University Press; 2014. doi:10.1093/med/9780199653461.003.0028. - DOI
-
- Walston J, Hadley EC, Ferrucci L, et al. Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J Am Geriatr Soc. Jun 2006;54(6):991–100, doi:10.1111/j.1532-5415.2006.00745.x. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
