

A New Concept of Using Femoral Condyles Surface for Femoral Component Alignment During Total Knee Arthroplasty: A Technical Note
- PMID: 38009183
- PMCID: PMC10673776
- DOI: 10.1007/s43465-023-01023-0
A New Concept of Using Femoral Condyles Surface for Femoral Component Alignment During Total Knee Arthroplasty: A Technical Note
Abstract
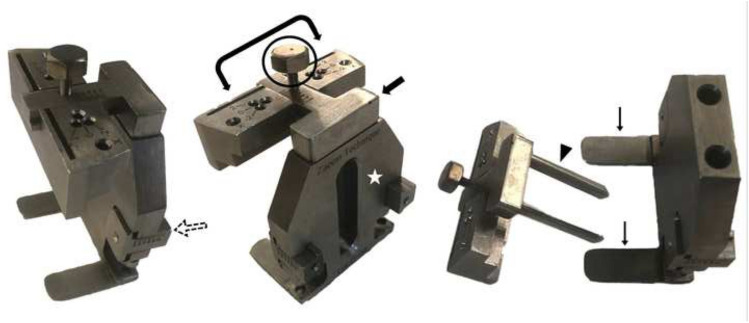
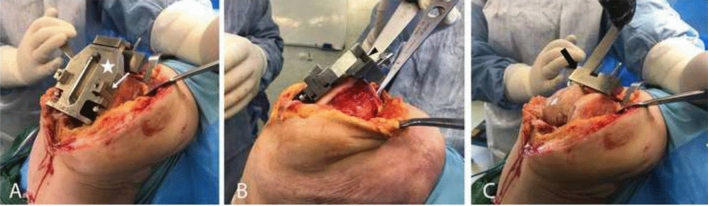
Background: Orthopedic surgeons favor an intramedullary guiding system on the femoral component during total knee arthroplasty (TKA); nevertheless, improper positioning of the entry point affects the final alignment. We have designed a new femoral cutting system for TKA that uses the distal and posterior femoral condyles as reference points for the setting of the cutting system regardless of the femoral canal. This study aims to evaluate the outcomes of this new guiding system.
Methods: We enrolled a series of 75 consecutive knees undergoing TKA. The alpha, gamma, and hip-knee-ankle (HKA) angles were assessed three months postoperatively. Also, surgical time and intraoperative blood loss were recorded for all patients.
Results: Fifteen patients underwent TKA using the mechanical alignment (MA) strategy, and 60 underwent kinematically aligned (KA) TKA. Both groups showed normal coronal and sagittal alignment 3 months postoperatively. The mean intraoperative blood loss was 213.11 ± 52.73 ml, which was not different between the two groups (n.s.). The mean surgical time was 43.12 ± 11.62 min, which was significantly shorter in the KA-TKA (41.11 ± 3.77 min) than in the MA-TKA (49.34 ± 4.56 min) (P < 0.001).
Conclusion: Using the new guiding system with good femoral alignment, we introduced the easily palpable and available condylar surface as a new landmark for cutting the distal femur in TKA.
Level of evidence: IV.
Keywords: Femoral alignment; Kinematic; Mechanical; Total knee arthroplasty.
© Indian Orthopaedics Association 2023. Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Conflict of interest statement
Conflict of InterestAll authors declared no conflict of interest.
Figures



Similar articles
-
Cementless, Cruciate-Retaining Primary Total Knee Arthroplasty Using Conventional Instrumentation: Technical Pearls and Intraoperative Considerations.JBJS Essent Surg Tech. 2024 Sep 13;14(3):e23.00036. doi: 10.2106/JBJS.ST.23.00036. eCollection 2024 Jul-Sep. JBJS Essent Surg Tech. 2024. PMID: 39280965 Free PMC article.
-
Deviations in femoral joint lines using calipered kinematically aligned TKA from virtually planned joint lines are small and do not affect clinical outcomes.Knee Surg Sports Traumatol Arthrosc. 2020 Oct;28(10):3118-3127. doi: 10.1007/s00167-019-05776-w. Epub 2019 Nov 25. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 31768572
-
An early clinical comparative study on total knee arthroplasty with kinematic alignment using specific instruments versus mechanical alignment in varus knees.Front Surg. 2023 Jan 18;9:1097302. doi: 10.3389/fsurg.2022.1097302. eCollection 2022. Front Surg. 2023. PMID: 36743893 Free PMC article.
-
Highly variable coronal tibial and femoral alignment in osteoarthritic knees: a systematic review.Knee Surg Sports Traumatol Arthrosc. 2019 May;27(5):1368-1377. doi: 10.1007/s00167-019-05506-2. Epub 2019 Apr 15. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 30989273
-
Comparison of Kinematic Alignment and Mechanical Alignment in Total Knee Arthroplasty: A Meta-analysis of Randomized Controlled Clinical Trials.Orthop Surg. 2020 Dec;12(6):1567-1578. doi: 10.1111/os.12826. Epub 2020 Oct 25. Orthop Surg. 2020. PMID: 33099892 Free PMC article. Review.
Cited by
-
One-Stage Primary Total Knee Arthroplasty as the Treatment of Acute Septic Arthritis of the Native Osteoarthritic Knee: Report of 3 Cases and Review of Literature.Arthroplast Today. 2025 Jul 28;34:101777. doi: 10.1016/j.artd.2025.101777. eCollection 2025 Aug. Arthroplast Today. 2025. PMID: 40761690 Free PMC article.
References
-
- Gøthesen Ø, Espehaug B, Havelin LI, Petursson G, Hallan G, Strøm E, et al. Functional outcome and alignment in computer-assisted and conventionally operated total knee replacements: A multicentre parallel-group randomised controlled trial. The bone & joint journal. 2014;96(5):609–618. doi: 10.1302/0301-620X.96B5.32516. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous