

Effect of Personalized Risk-Reduction Strategies on Cognition and Dementia Risk Profile Among Older Adults: The SMARRT Randomized Clinical Trial
- PMID: 38010725
- PMCID: PMC10682943
- DOI: 10.1001/jamainternmed.2023.6279
Effect of Personalized Risk-Reduction Strategies on Cognition and Dementia Risk Profile Among Older Adults: The SMARRT Randomized Clinical Trial
Abstract
Importance: Modifiable risk factors are hypothesized to account for 30% to 40% of dementia; yet, few trials have demonstrated that risk-reduction interventions, especially multidomain, are efficacious.
Objective: To determine if a personalized, multidomain risk reduction intervention improves cognition and dementia risk profile among older adults.
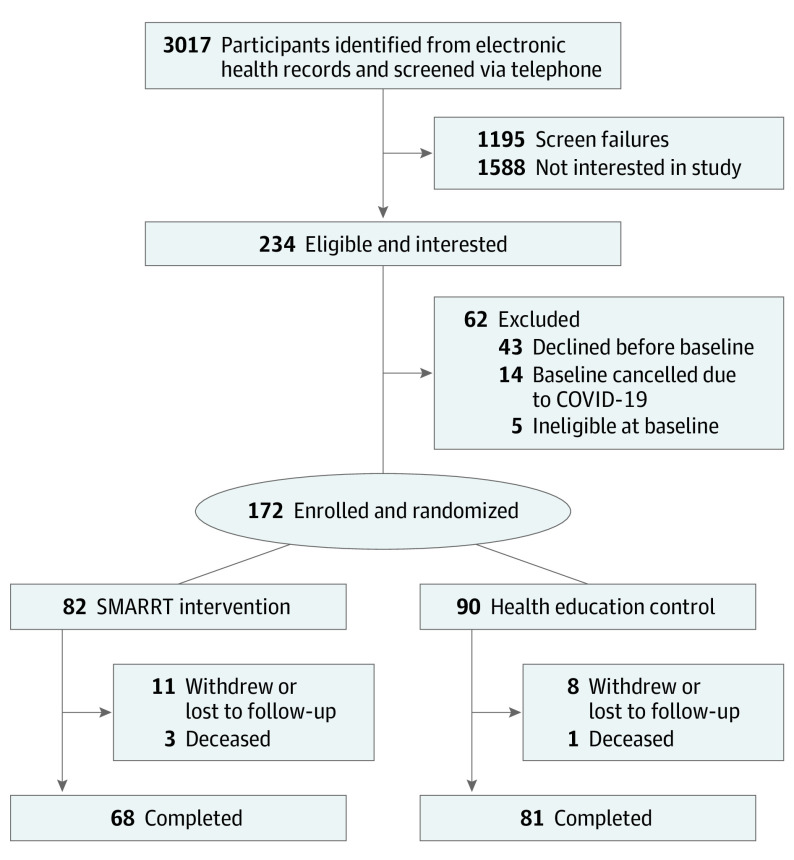
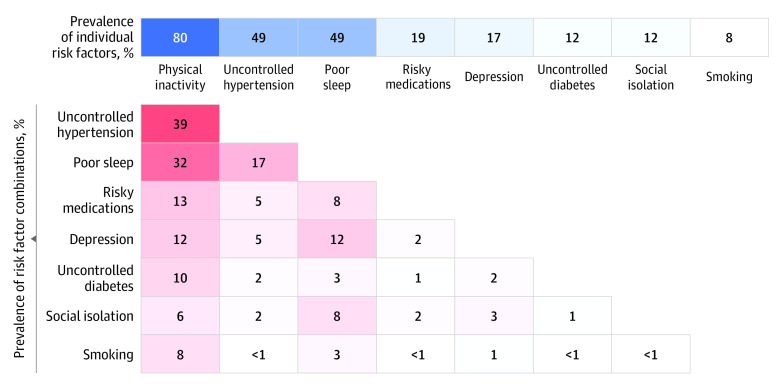
Design, setting, and participants: The Systematic Multi-Domain Alzheimer Risk Reduction Trial was a randomized clinical trial with a 2-year personalized, risk-reduction intervention. A total of 172 adults at elevated risk for dementia (age 70-89 years and with ≥2 of 8 targeted risk factors) were recruited from primary care clinics associated with Kaiser Permanente Washington. Data were collected from August 2018 to August 2022 and analyzed from October 2022 to September 2023.
Intervention: Participants were randomly assigned to the intervention (personalized risk-reduction goals with health coaching and nurse visits) or to a health education control.
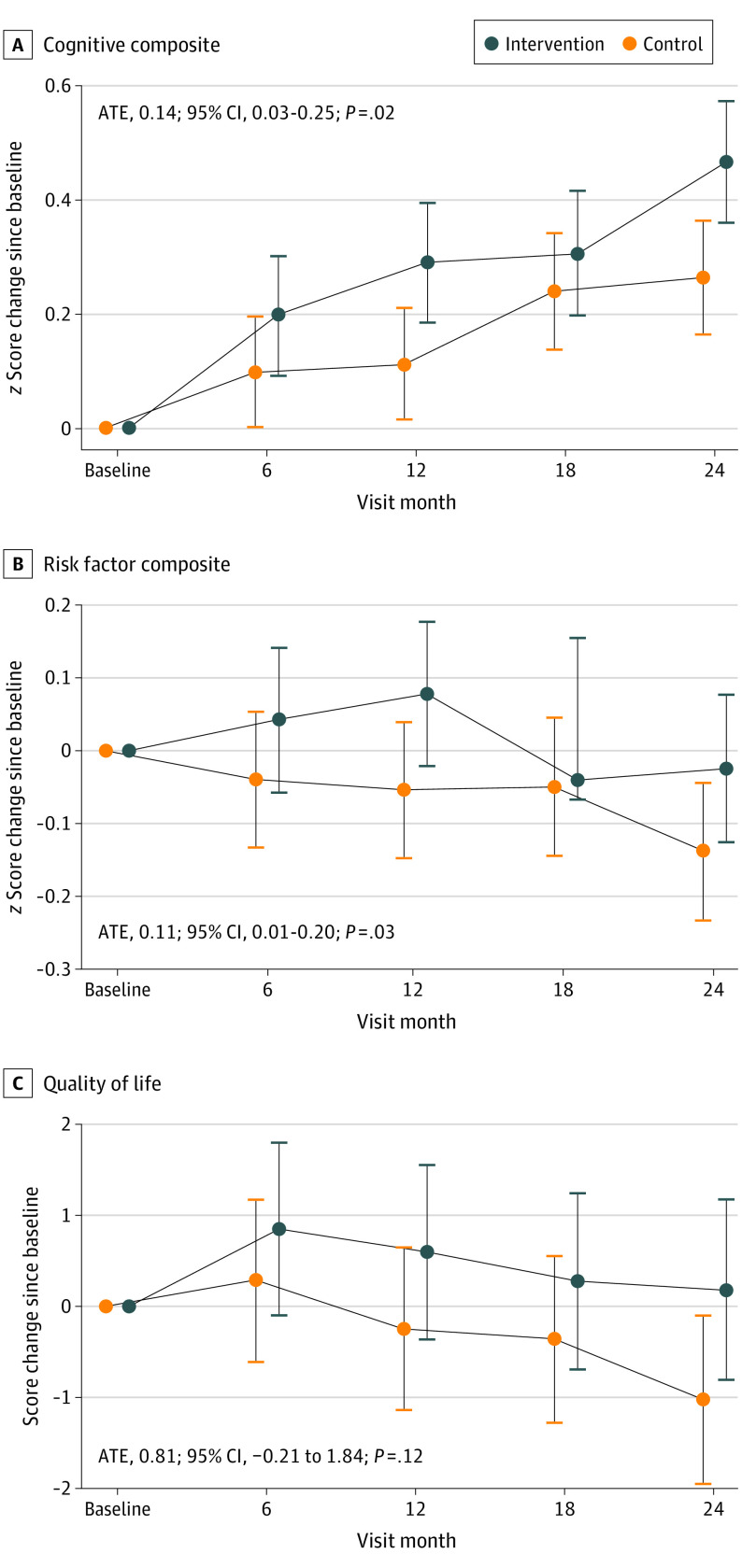
Main outcomes and measures: The primary outcome was change in a composite modified Neuropsychological Test Battery; preplanned secondary outcomes were change in risk factors and quality of life (QOL). Outcomes were assessed at baseline and 6, 12, 18, and 24 months. Linear mixed models were used to compare, by intention to treat, average treatment effects (ATEs) from baseline over follow-up. The intervention and outcomes were initially in person but then, due to onset of the COVID-19 pandemic, were remote.
Results: The 172 total participants had a mean (SD) age of 75.7 (4.8) years, and 108 (62.8%) were women. After 2 years, compared with the 90 participants in the control group, the 82 participants assigned to intervention demonstrated larger improvements in the composite cognitive score (ATE of SD, 0.14; 95% CI, 0.03-0.25; P = .02; a 74% improvement compared with the change in the control group), better composite risk factor score (ATE of SD, 0.11; 95% CI, 0.01-0.20; P = .03), and improved QOL (ATE, 0.81 points; 95% CI, -0.21 to 1.84; P = .12). There were no between-group differences in serious adverse events (24 in the intervention group and 23 in the control group; P = .59), but the intervention group had greater treatment-related adverse events such as musculoskeletal pain (14 in the intervention group vs 0 in the control group; P < .001).
Conclusions and relevance: In this randomized clinical trial, a 2-year, personalized, multidomain intervention led to modest improvements in cognition, dementia risk factors, and QOL. Modifiable risk-reduction strategies should be considered for older adults at risk for dementia.
Trial registration: ClinicalTrials.gov Identifier: NCT03683394.
Conflict of interest statement
Figures
References
-
- Mehegan L, Rainville C. 2021 AARP survey on the perceptions related to a dementia diagnosis: adults age 40-plus. AARP . June 22, 2021. Accessed October 20, 2023. https://www.aarp.org/content/dam/aarp/research/surveys_statistics/health...
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
