

Real-world treatment outcome of direct-acting antivirals and patient survival rates in chronic hepatitis C virus infection in Eritrea
- PMID: 38012181
- PMCID: PMC10682448
- DOI: 10.1038/s41598-023-47258-7
Real-world treatment outcome of direct-acting antivirals and patient survival rates in chronic hepatitis C virus infection in Eritrea
Abstract
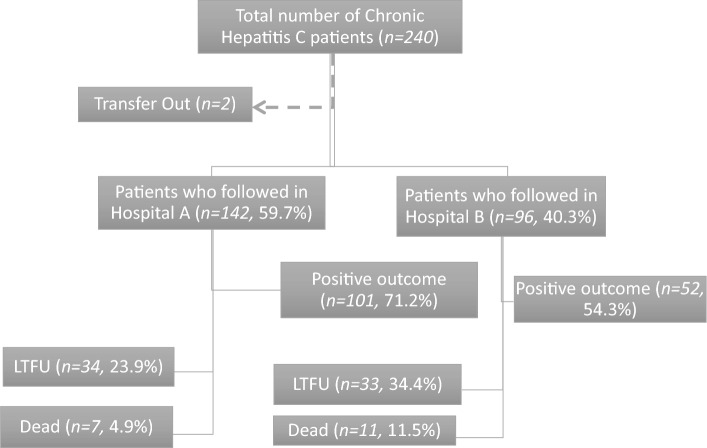
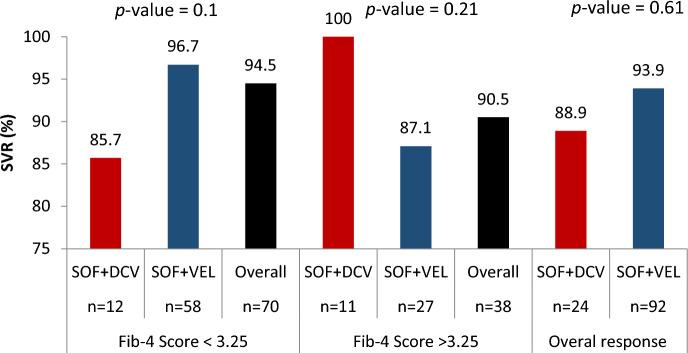
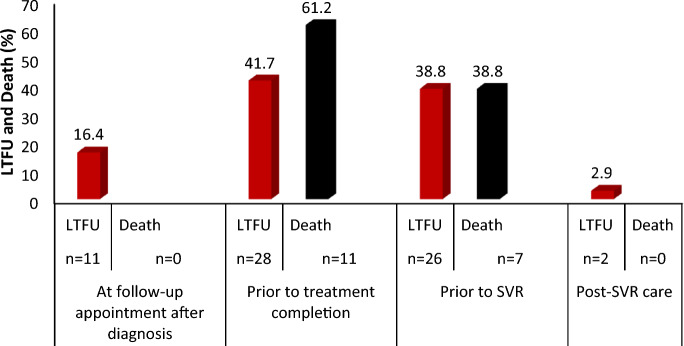
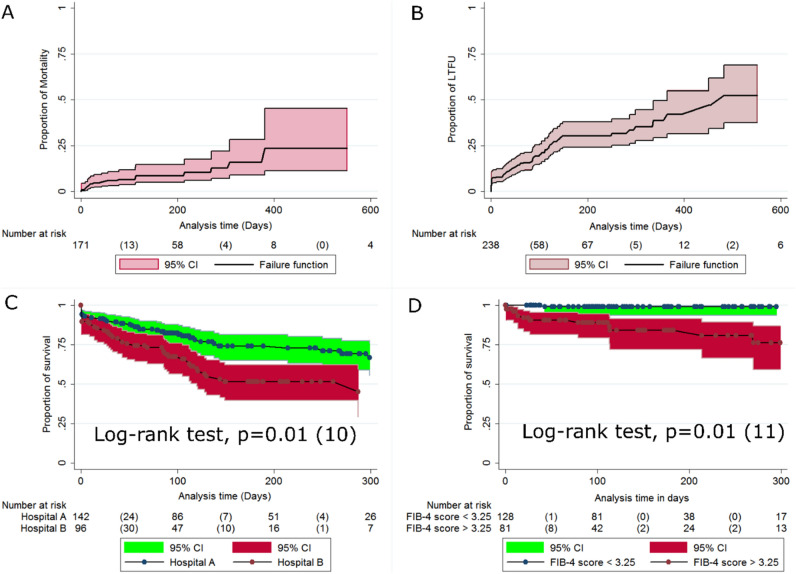
Reliable real-world data on direct acting anti-retroviral (DAA) uptake and treatment outcomes are lacking for patients with hepatitis C virus (HCV) in sub-Saharan Africa. This study provides data on HCV DAA-based treatment outcomes, mortality, loss-to-follow up, and associated factors among patients in Eritrea. A multicenter retrospective observational cohort study was conducted in two tertiary hospitals in Asmara, Eritrea. A structured checklist was used to collect data from patient's cards. Descriptive and inferential statistics used included means (± Standard deviation (SD), medians (Interquartile range (IQR), chi-squire (χ2), Kaplan-Meier estimates, and multivariate Cox proportional hazard models. A total of 238 patients with median age of 59 years (IQR 50-69 years) were enrolled in the study. Out of the 227 patients initiated on treatment, 125 patients had viral load measurements at 12 weeks after end of treatment (EOT) whereas 102 patients had no viral load measurements at 12 weeks EOT. Among the patients with HCV RNA data post-EOT 12, 116 (92.8%) had sustained viral response (SVR). The prevalence of death and loss-to-follow up (LTFU) were (7.5%, 95% CI 1.7-4.1) and 67 (28.1%, 95% CI 22.3-33.9) translating into an incidence of 1.1 (95% CI 0.8-1.5) per 10,000 person days. Independent predictors of LTFU included the enrollment year (2020: aHR = 2.2, 95% CI 1-4.7; p value = 0.04); Hospital (Hospital B: aHR = 2.2, 95% CI 1-4.7; p value = 0.03) and the FIB-4 score (FIB-Score < 1.45: aHR = 3.7, 95% CI 1.2-11.5; p value = 0.02). The SVR rates achieved in this cohort were high. However, high LTFU and high mortality driven largely by late presentation and suboptimal population screening/case finding, were uncovered. These challenges can be addressed by test-and-treat programs that simultaneously prioritize programmatic screening, decentralization of care, and better patient tracking in the HCV care cascade.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Real-world experience with nucleos(t)ide analogue therapy and patient survival rates in chronic viral hepatitis B treatment centers in Eritrea.Sci Rep. 2025 Jan 4;15(1):824. doi: 10.1038/s41598-024-79600-y. Sci Rep. 2025. PMID: 39755688 Free PMC article.
-
Hepatocellular carcinoma, decompensation, and mortality based on hepatitis C treatment: A prospective cohort study.World J Gastroenterol. 2022 Aug 14;28(30):4182-4200. doi: 10.3748/wjg.v28.i30.4182. World J Gastroenterol. 2022. PMID: 36157119 Free PMC article.
-
Prevalence and factors associated with pediatric HIV therapy failure in a tertiary hospital in Asmara, Eritrea: A 15-year retrospective cohort study.PLoS One. 2023 Mar 9;18(3):e0282642. doi: 10.1371/journal.pone.0282642. eCollection 2023. PLoS One. 2023. PMID: 36893200 Free PMC article.
-
Direct-acting antiviral treatment of chronic HCV-infected patients on opioid substitution therapy: Still a concern in clinical practice?Addiction. 2018 May;113(5):868-882. doi: 10.1111/add.14128. Epub 2018 Jan 23. Addiction. 2018. PMID: 29359361
-
Loss to follow-up in the hepatitis C care cascade: A substantial problem but opportunity for micro-elimination.J Viral Hepat. 2020 Dec;27(12):1270-1283. doi: 10.1111/jvh.13399. Epub 2020 Sep 22. J Viral Hepat. 2020. PMID: 32964615 Free PMC article. Review.
Cited by
-
An unusual survival for 6.5 years with end-stage hepatitis C related advanced liver cirrhosis following sustained virologic response with direct antiviral agents - A case report from A low-resource setting.Niger Med J. 2025 Jun 16;66(2):791-798. doi: 10.71480/nmj.v66i2.661. eCollection 2025 Mar-Apr. Niger Med J. 2025. PMID: 40703894 Free PMC article.
-
Treatment outcomes of chronic liver disease and associated factors among patients treated at hospitals in Bahir Dar city, north-west Ethiopia.BMC Gastroenterol. 2025 Mar 6;25(1):141. doi: 10.1186/s12876-025-03719-z. BMC Gastroenterol. 2025. PMID: 40050738 Free PMC article.
References
-
- World Health Organization. Global hepatitis report 2017, https://www.who.int/hepatitis/publications/global-hepatitis-report2017/en/ (2017).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
