

Causal inference using observational intensive care unit data: a scoping review and recommendations for future practice
- PMID: 38012221
- PMCID: PMC10682453
- DOI: 10.1038/s41746-023-00961-1
Causal inference using observational intensive care unit data: a scoping review and recommendations for future practice
Abstract
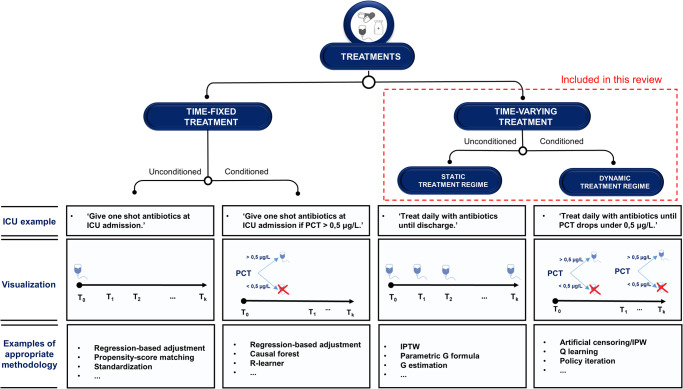
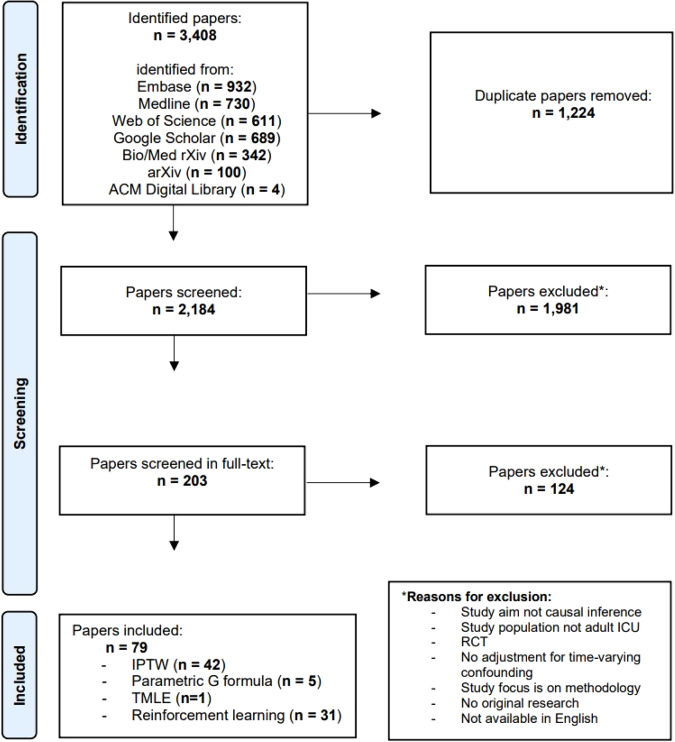
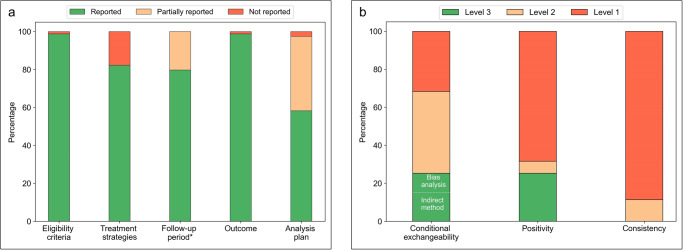
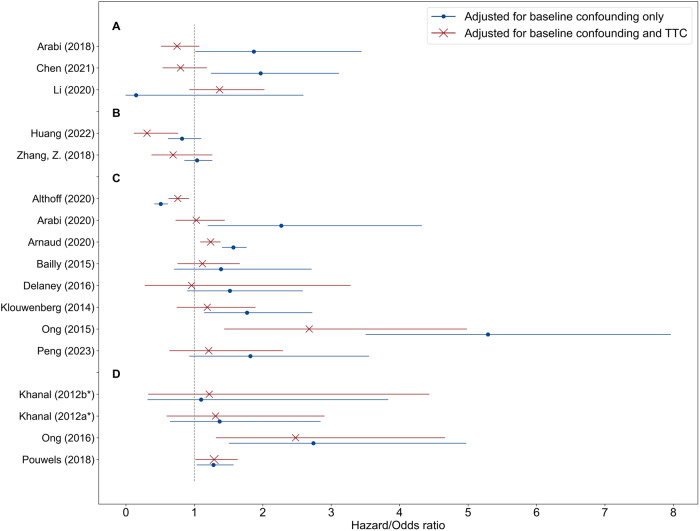
This scoping review focuses on the essential role of models for causal inference in shaping actionable artificial intelligence (AI) designed to aid clinicians in decision-making. The objective was to identify and evaluate the reporting quality of studies introducing models for causal inference in intensive care units (ICUs), and to provide recommendations to improve the future landscape of research practices in this domain. To achieve this, we searched various databases including Embase, MEDLINE ALL, Web of Science Core Collection, Google Scholar, medRxiv, bioRxiv, arXiv, and the ACM Digital Library. Studies involving models for causal inference addressing time-varying treatments in the adult ICU were reviewed. Data extraction encompassed the study settings and methodologies applied. Furthermore, we assessed reporting quality of target trial components (i.e., eligibility criteria, treatment strategies, follow-up period, outcome, and analysis plan) and main causal assumptions (i.e., conditional exchangeability, positivity, and consistency). Among the 2184 titles screened, 79 studies met the inclusion criteria. The methodologies used were G methods (61%) and reinforcement learning methods (39%). Studies considered both static (51%) and dynamic treatment regimes (49%). Only 30 (38%) of the studies reported all five target trial components, and only seven (9%) studies mentioned all three causal assumptions. To achieve actionable AI in the ICU, we advocate careful consideration of the causal question of interest, describing this research question as a target trial emulation, usage of appropriate causal inference methods, and acknowledgement (and examination of potential violations of) the causal assumptions.
© 2023. The Author(s).
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
