

The value of preoperative neutrophil/lymphocyte ratio in predicting the severity of cholecystolithiasis with cholecystitis in elderly patients
- PMID: 38012600
- PMCID: PMC10683304
- DOI: 10.1186/s12893-023-02267-1
The value of preoperative neutrophil/lymphocyte ratio in predicting the severity of cholecystolithiasis with cholecystitis in elderly patients
Abstract
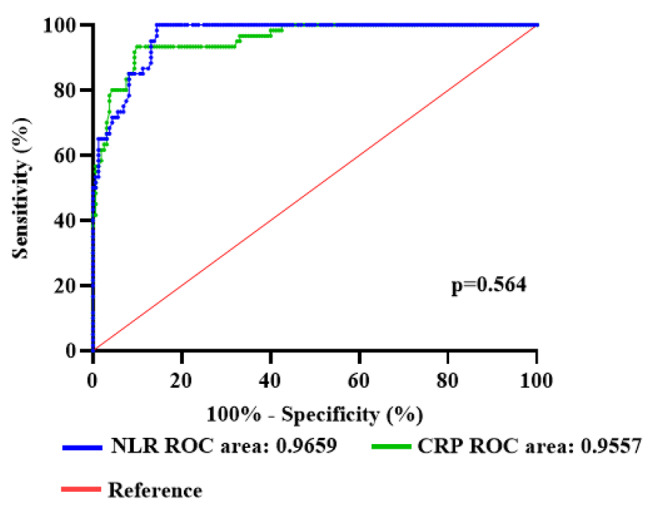
Background: This study aims to assess the effectiveness of neutrophil/lymphocyte ratio (NLR) and C-reactive protein (CRP) in diagnosing cholecystolithiasis with cholecystitis in elderly patients. Additionally, the study seeks to determine the predictive value of preoperative NLR in determining the severity of the condition in this population.
Methods: This study is a retrospective cohort study, including 160 elderly patients with cholecystolithiasis with cholecystitis (45 cases of simple cholecystitis, 58 cases of suppurative cholecystitis, 57 cases of gangrenous cholecystitis) and 60 cases of normal gallbladder histology. The study collected clinical data of the patients detected the preoperative CRP content, neutrophil, and lymphocyte levels through blood routine tests, and calculated the NLR value. The diagnostic value of NLR and CRP was determined by using the Receiver Operating Characteristic Curve (ROC), and the optimal value of preoperative NLR related to the severity of elderly patients with cholecystolithiasis with cholecystitis was identified.
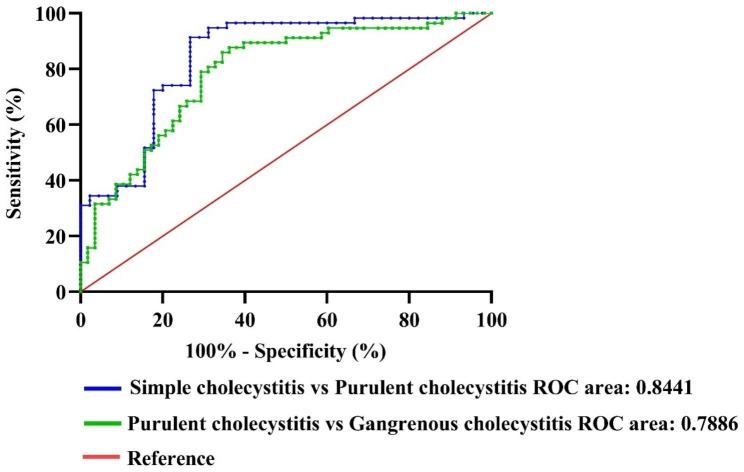
Results: This study found that for elderly patients with cholecystolithiasis with cholecystitis, preoperative NLR and CRP levels can be used to distinguish the condition. The critical value for NLR was found to be 2.995 (95% CI, 0.9465-0.9853; P < 0.001) with an area under the ROC curve of 0.9659, while the critical value for CRP was 13.05 (95% CI, 0.9284-0.9830; P < 0.001) with an area under the ROC curve of 0.9557. Both NLR and CRP were found to have equivalent diagnostic abilities. Additionally, the study found that there were significant differences in neutrophil and lymphocyte levels in elderly patients with different severity levels, with NLR increasing as severity increased (P < 0.001). The study identified cut-off values for preoperative NLR that could distinguish Simple cholecystitis and Purulent cholecystitis, as well as Purulent cholecystitis and Gangrenous cholecystitis in elderly patients with cholecystolithiasis, with respective AUCs of 0.8441 (95% CI: 0.7642-0.9239; P < 0.001) and 0.7886(95% CI: 0.7050-0.8721, P < 0.001), sensitivities of 91.38% and 87.72%, and specificities of 73.33% and 63.79%.
Conclusions: Preoperative NLR and CRP values can serve as indicators to detect cholecystolithiasis with cholecystitis in elderly patients. Additionally, NLR has been recognized as a potential tool to differentiate the severity of cholecystolithiasis with cholecystitis in the elderly population.
Keywords: C-reactive protein; Diagnosis; Inflammatory biomarkers; Neutrophil-to-lymphocyte ratio; Severity of cholecystolithiasis with cholecystitis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
