

Efficacy and Safety of Single-dose Pegfilgrastim for CD34 + Cell Mobilization in Healthy Volunteers: A Phase 2 Study
- PMID: 38012835
- PMCID: PMC10962423
- DOI: 10.1097/TP.0000000000004880
Efficacy and Safety of Single-dose Pegfilgrastim for CD34 + Cell Mobilization in Healthy Volunteers: A Phase 2 Study
Abstract
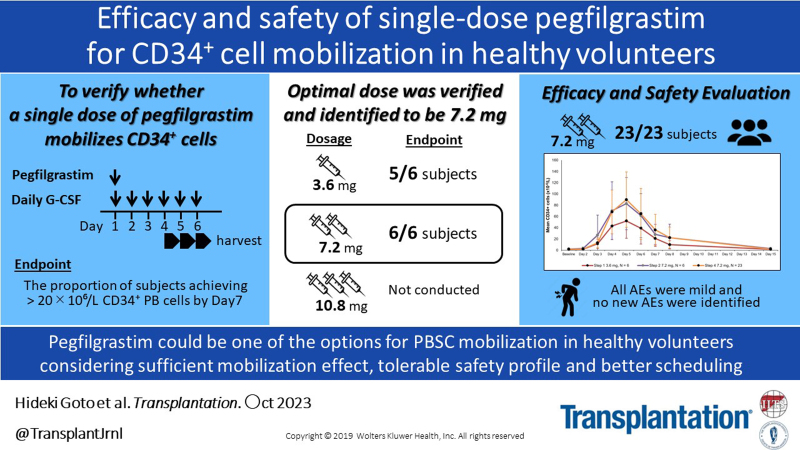
Background: Pegfilgrastim, a long-acting form of granulocyte-colony stimulating factor, with a convenient single-injection dosage, is being investigated for peripheral blood stem cell (PBSC) mobilization in healthy volunteers. However, data on the adequate dose of pegfilgrastim for PBSC mobilization are limited. This phase 2, single-arm study evaluated the efficacy and safety of pegfilgrastim for PBSC mobilization in healthy volunteers.
Methods: The study comprised 2 phases: pilot (steps 1-3, dose escalation, a single subcutaneous dose of 3.6, 7.2, and 10.8 mg pegfilgrastim, respectively) and evaluation (step 4, efficacy and safety assessments). The primary endpoint was the proportion of subjects who achieved mobilization of ≥20 × 10 6 /L cluster of differentiation 34 positive (CD34 + ) cells.
Results: Thirty-five subjects (6 each in steps 1 and 2 and 23 in step 4) were included. In the pilot phase, step 3 with a 10.8 mg dose was not conducted due to favorable outcomes in step 2 (desired CD34 + cell count), at 7.2 mg pegfilgrastim, which was identified as the optimal dose for the evaluation phase. In the evaluation phase, successful CD34 + mobilization was achieved in all 23 subjects. The mean peripheral blood CD34 + cells count peaked on day 5. Back pain, thrombocytopenia, transient elevations of alkaline phosphatase, and lactate dehydrogenase were the most common adverse events. All adverse events were mild, and none led to study discontinuation.
Conclusions: A single-dose pegfilgrastim successfully mobilized an optimal number of CD34 + cells and was well tolerated. Pegfilgrastim could be an alternative option for PBSC mobilization in healthy volunteers. The trial was registered at www.clinicaltrials.gov (NCT03993639).
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Y.I. and M.O. are employees of Kyowa Kirin Co Ltd. These authors have received research funds/grants/incentives/endowments: H.G. from Chugai and Novartis, Bristol-Myers Squibb, Symbio, and Kyowa Kirin; M.N. from Nippon Shinyaku; M.H. from Kyowa Kirin and Chugai; Y.M. from Kyowa Kirin; and T.T. from AbbVie, Astellas, Nippon Shinyaku, Novartis, Bristol-Myers Squibb, Sumitomo Pharma, Merck Sharp & Dohme, Celgene, Chugai, Janssen, Fuji Pharma, Asahi Kasei Pharma, Eisai, Sumitomo Pharma, ONO, Astellas, Shionogi, Priothera SAS, LUCA Science, Kyowa Kirin, and Otsuka. The other authors declare no conflicts of interest.
Figures




References
-
- Copelan EA, Chojecki A, Lazarus HM, et al. . Allogeneic hematopoietic cell transplantation; the current renaissance. Blood Rev. 2019;34:34–44. - PubMed
-
- Rowley SD, Donaldson G, Lilleby K, et al. . Experiences of donors enrolled in a randomized study of allogeneic bone marrow or peripheral blood stem cell transplantation. Blood. 2001;97:2541–2548. - PubMed
-
- Richard EC, Norbert S, Mary M, et al. . Blood stem cells compared with bone marrow as a source of hematopoietic cells for allogeneic transplantation. Blood. 2000;95:3702–3709. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
