

The impact of margin reduction on radiation dose distribution of ultra-hypofractionated prostate radiotherapy utilizing a 1.5-T MR-Linac
- PMID: 38013636
- PMCID: PMC10795449
- DOI: 10.1002/acm2.14179
The impact of margin reduction on radiation dose distribution of ultra-hypofractionated prostate radiotherapy utilizing a 1.5-T MR-Linac
Abstract
Background: We examined the effects of reducing the planning target volume (PTV) margin in MR-guided radiotherapy (MRgRT) on the distribution of radiation dose to target volumes and organs-at-risk (OARs). Thus, we compared MR-Linac (MRL) plans with and without reduced margin and intensity-modulated radiotherapy (IMRT) plan with conventional linac for low-risk prostate cancer patients receiving 36.25 Gy in five fractions of ultra-hypofractionated radiation therapy.
Materials and methods: Twenty low-risk prostate cancer patients treated with 1.5 T MR-Linac were evaluated. The same planning CT images were used for four plans: the MRL-R plan with reduced margin planning target volume (PTV-R) and the MRL-N plan with normal margin PTV (PTV-N), which is also used for IMRT plan. In four plans, PTV doses, organs-at-risk (OARs) doses, the homogeneity index (HI), and monitor units were compared.
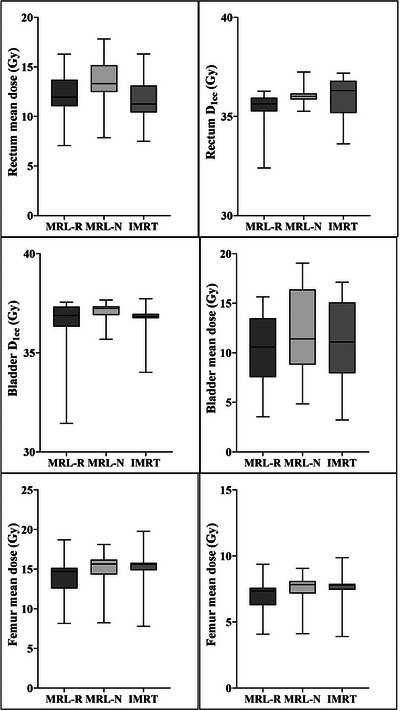
Results: All plans met the criteria for PTV coverage and OARs dose constraints. The maximum and mean PTV doses were significantly higher in the MRL-R and MRL-N plans compared to the IMRT plan. The HI was lowest in the IMRT plan (0.040 ± 0.013) and highest in the MRL-N plan (0.055 ± 0.012; p < 0.001). There was no significant difference in the PTV dosimetric parameters between the MRL-R and the MRL-N plans. The high doses in the rectum was significantly lower in the MRL-R compared to other plans. The bladder V36.25 Gy was significantly lower in the MRL-R plan (2.43 ± 1.87 Gy) compared to MRL-N (4.50 ± 2.42 Gy; p < 0.001), and IMRT plans (4.76 ± 2.77 Gy; p < 0.001). There was no significant difference in the low-dose volumes of the body, maximum femur doses, or monitor units across each plan.
Conclusions: Ultra-hypofractionated MR-guided RT with 1.5 T MRL is dosimetrically feasible for patients with prostate cancer. The improved soft tissue contrast and the online adaptive plan for 1.5 T MR-Linac allows for PTV margin reduction resulted in a significant dose reduction in OARs.
Keywords: MR-linac; dosimetry; prostate cancer; radiotherapy; stereotactic body radiotherapy.
© 2023 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals LLC on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures



References
-
- Lagendijk JJ, Raaymakers BW, Raaijmakers AJ, et al. MRI/linac integration. Radiother Oncol. 2008;86(1):25‐29. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
