

This is a preprint.
Application of machine learning models to identify serological predictors of COVID-19 severity and outcomes
- PMID: 38014049
- PMCID: PMC10680931
- DOI: 10.21203/rs.3.rs-3463155/v1
Application of machine learning models to identify serological predictors of COVID-19 severity and outcomes
Update in
-
Application of machine learning algorithms to identify serological predictors of COVID-19 severity and outcomes.Commun Med (Lond). 2024 Nov 26;4(1):249. doi: 10.1038/s43856-024-00658-w. Commun Med (Lond). 2024. PMID: 39592832 Free PMC article.
Abstract
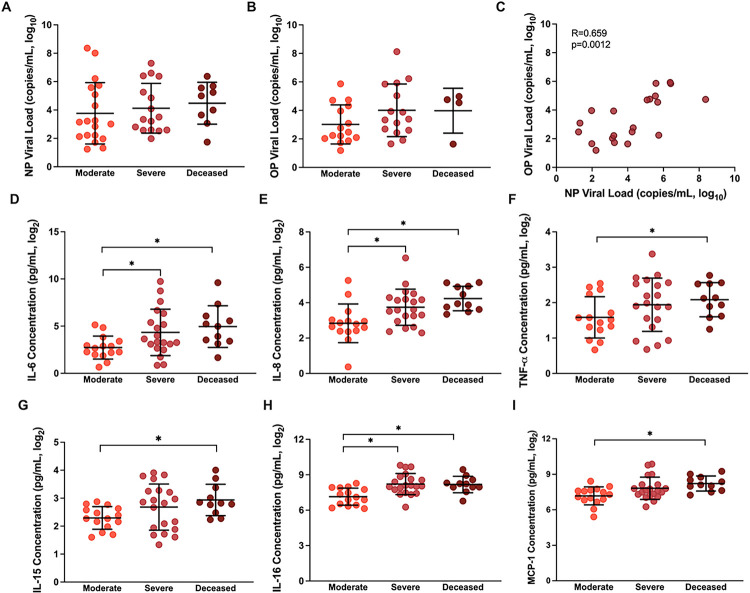
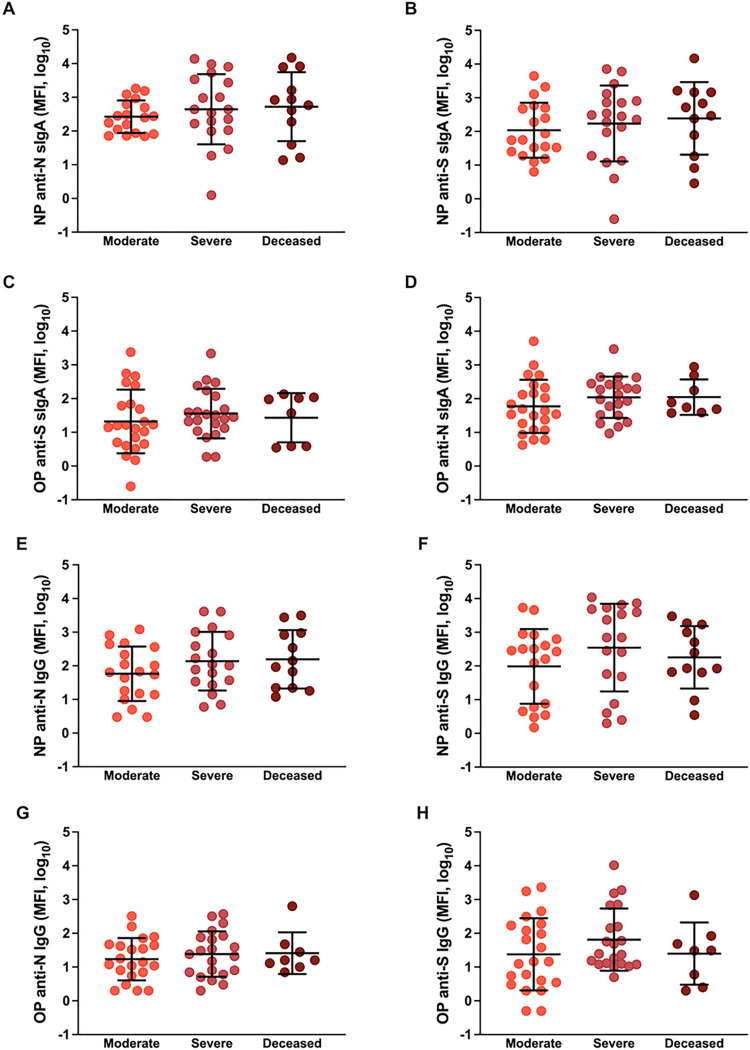
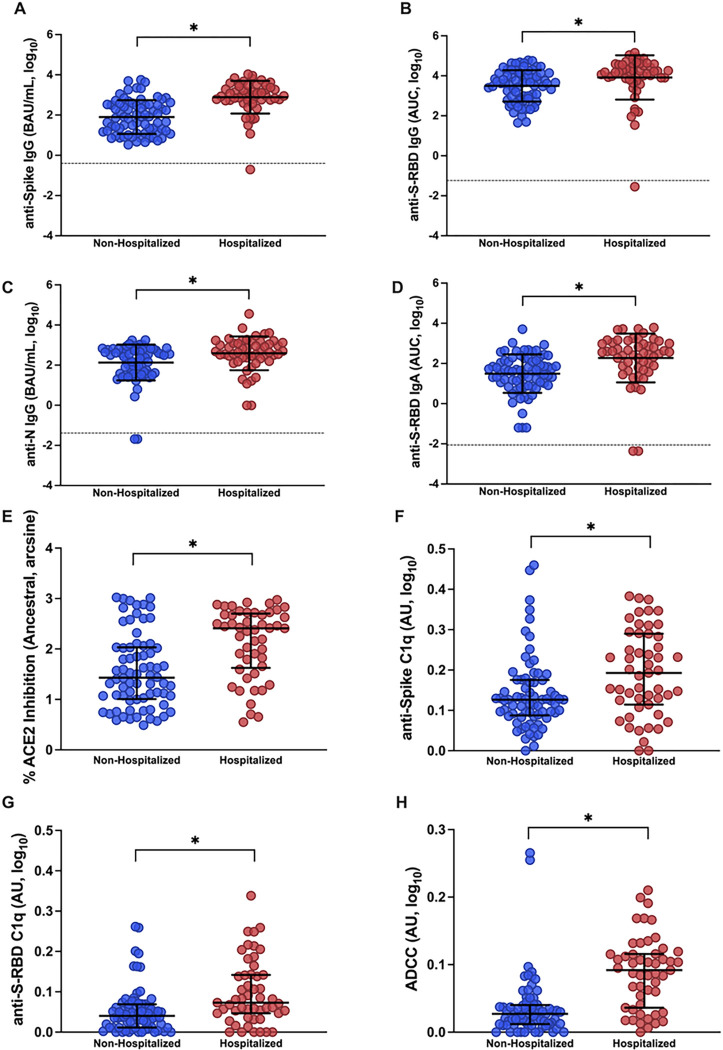
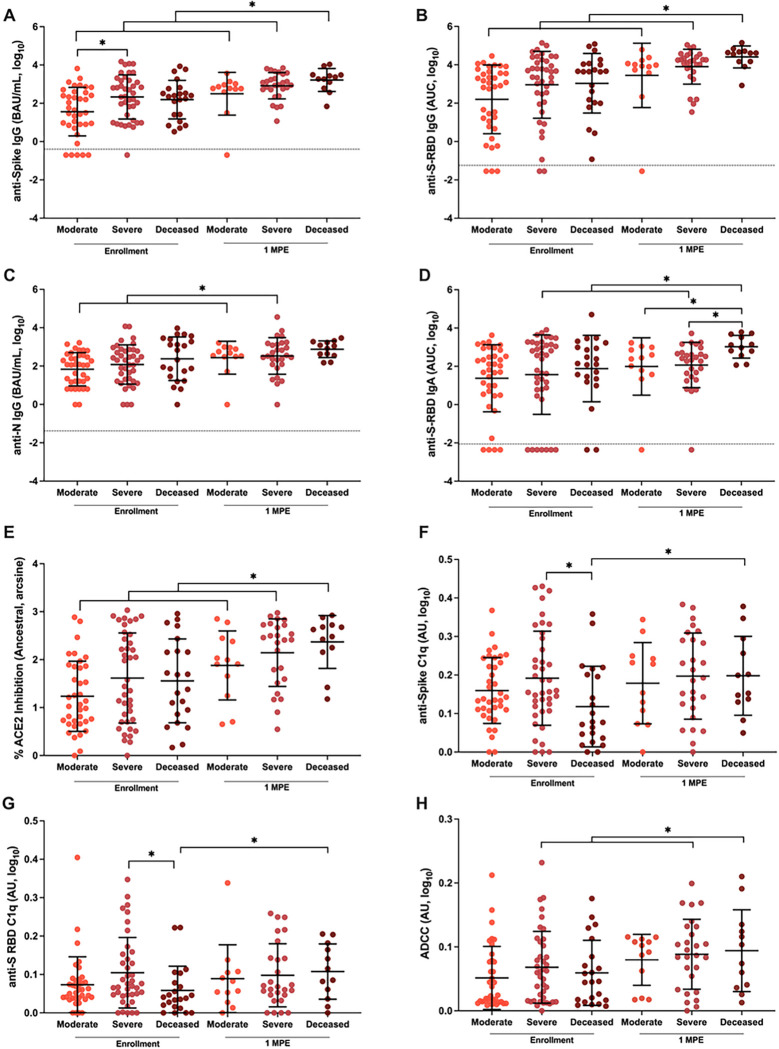
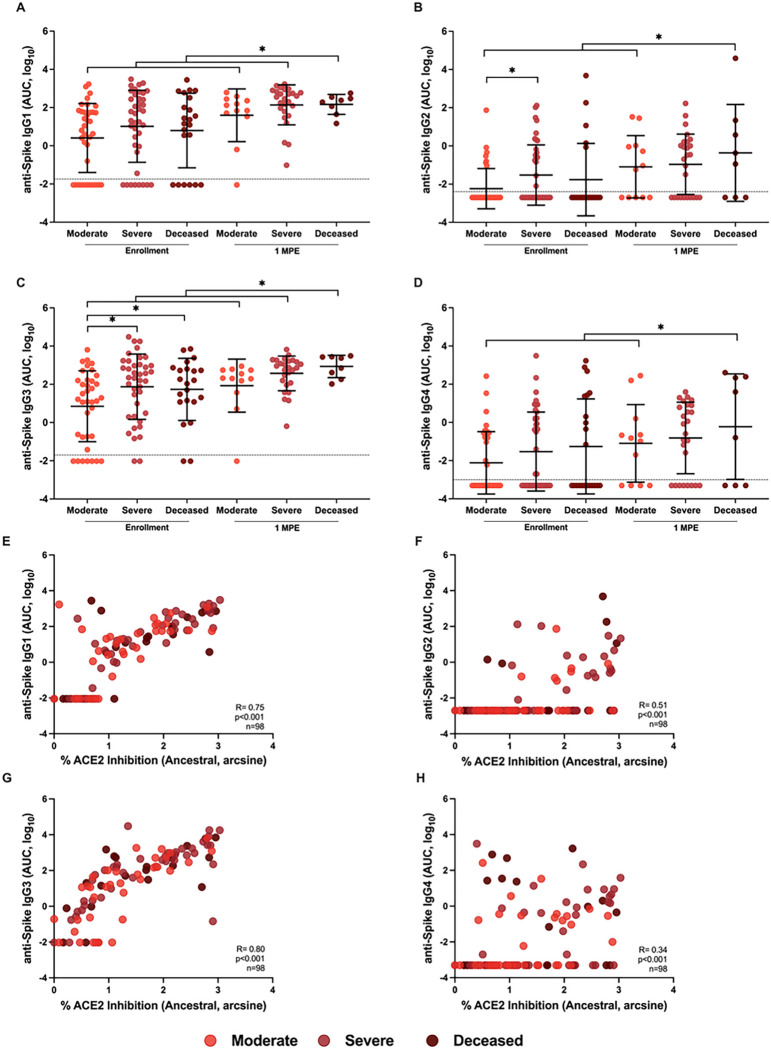
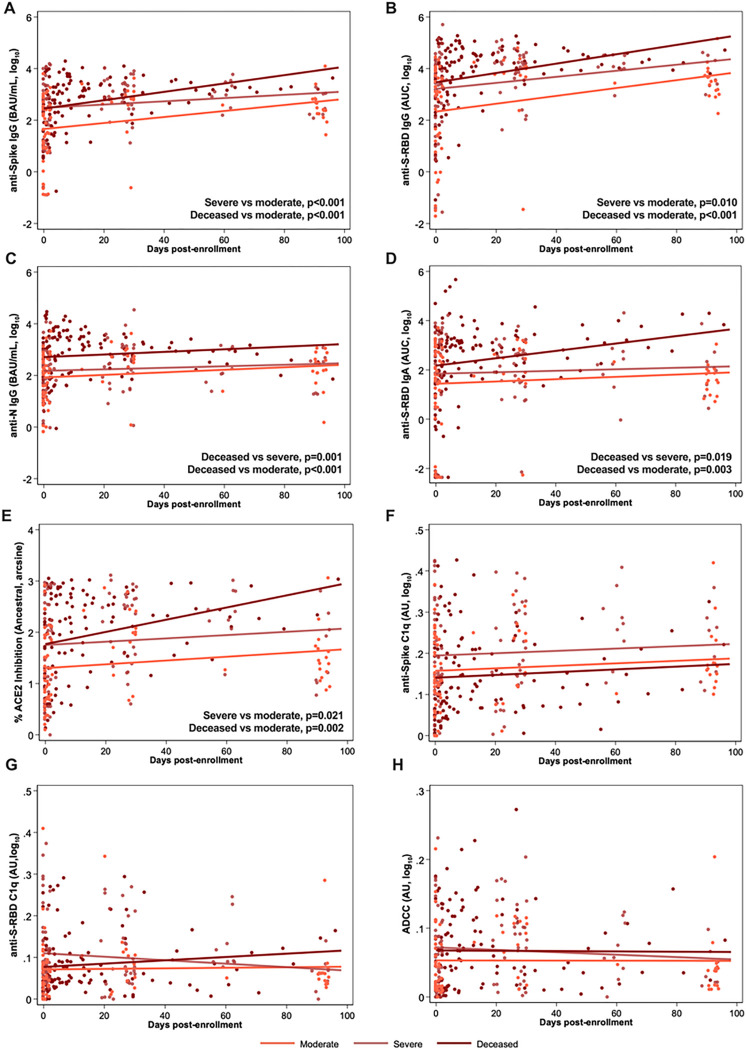
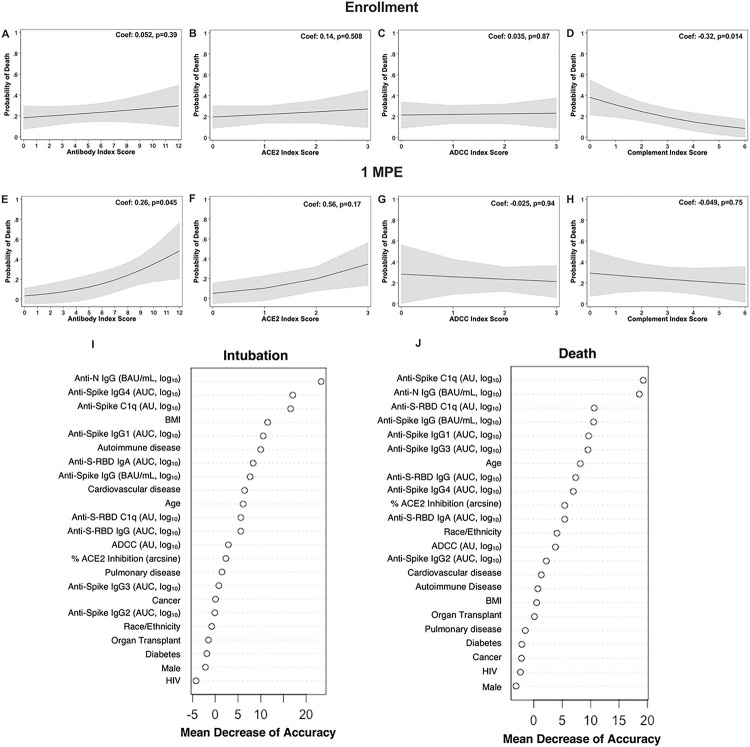
Critically ill people with COVID-19 have greater antibody titers than those with mild to moderate illness, but their association with recovery or death from COVID-19 has not been characterized. In 178 COVID-19 patients, 73 non-hospitalized and 105 hospitalized patients, mucosal swabs and plasma samples were collected at hospital enrollment and up to 3 months post-enrollment (MPE) to measure virus RNA, cytokines/chemokines, binding antibodies, ACE2 binding inhibition, and Fc effector antibody responses against SARS-CoV-2. The association of demographic variables and >20 serological antibody measures with intubation or death due to COVID-19 was determined using machine learning algorithms. Predictive models revealed that IgG binding and ACE2 binding inhibition responses at 1 MPE were positively and C1q complement activity at enrollment was negatively associated with an increased probability of intubation or death from COVID-19 within 3 MPE. Serological antibody measures were more predictive than demographic variables of intubation or death among COVID-19 patients.
Keywords: COVID-19 death; COVID-19 hospitalization; IgG isotypes; automated intelligence; neutralizing antibody; non-neutralizing antibody; random forest model.
Conflict of interest statement
Conflicts of interest The authors declare no conflicts of interest.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
