

Early Serial Echocardiographic and Ultrasonographic Findings in Critically Ill Patients With COVID-19
- PMID: 38014378
- PMCID: PMC10030437
- DOI: 10.1016/j.chstcc.2023.100002
Early Serial Echocardiographic and Ultrasonographic Findings in Critically Ill Patients With COVID-19
Abstract
Background: Cardiac function of critically ill patients with COVID-19 generally has been reported from clinically obtained data. Echocardiographic deformation imaging can identify ventricular dysfunction missed by traditional echocardiographic assessment.
Research question: What is the prevalence of ventricular dysfunction and what are its implications for the natural history of critical COVID-19?
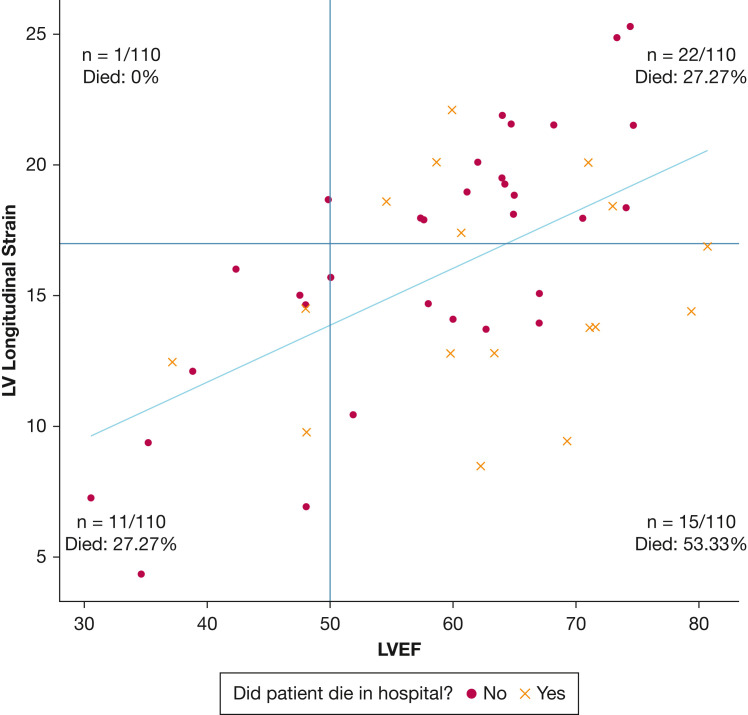
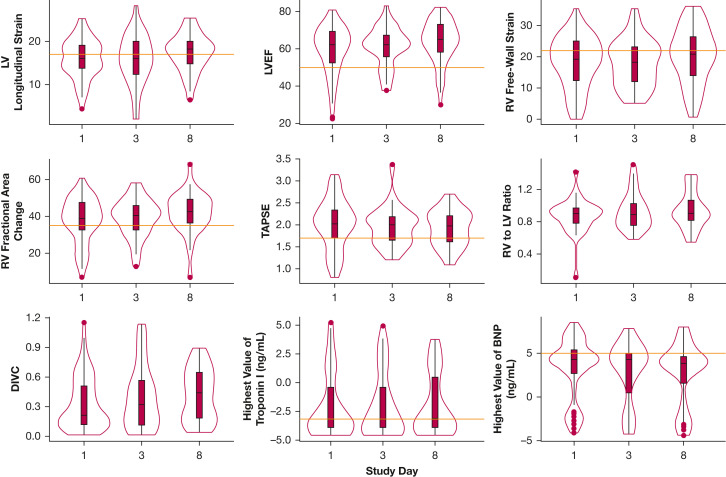
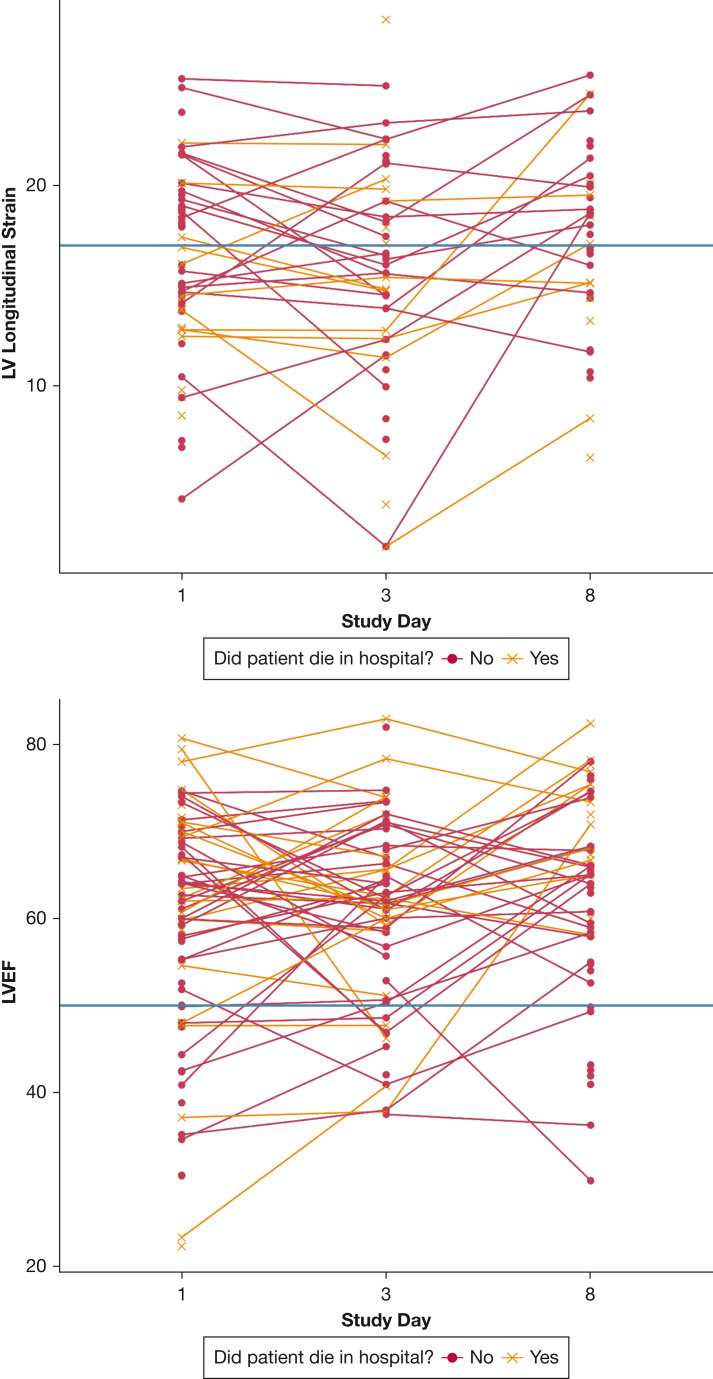
Study design and methods: This is a multicenter prospective cohort of critically ill patients with COVID-19. We performed serial echocardiography and lower extremity vascular ultrasound on hospitalization days 1, 3, and 8. We defined left ventricular (LV) dysfunction as the absolute value of longitudinal strain of < 17% or left ventricle ejection fraction (LVEF) of < 50%. Primary clinical outcome was inpatient survival.
Results: We enrolled 110 patients. Thirty-nine (35.5%) died before hospital discharge. LV dysfunction was present at admission in 38 patients (34.5%) and in 21 patients (36.2%) on day 8 (P = .59). Median baseline LVEF was 62% (interquartile range [IQR], 52%-69%), whereas median absolute value of baseline LV strain was 16% (IQR, 14%-19%). Survivors and nonsurvivors did not differ statistically significantly with respect to day 1 LV strain (17.9% vs 14.4%; P = .12) or day 1 LVEF (60.5% vs 65%; P = .06). Nonsurvivors showed worse day 1 right ventricle (RV) strain than survivors (16.3% vs 21.2%; P = .04).
Interpretation: Among patients with critical COVID-19, LV and RV dysfunction is common, frequently identified only through deformation imaging, and early (day 1) RV dysfunction may be associated with clinical outcome.
Keywords: COVID-19; echocardiography; point-of-care ultrasound; strain; ultrasound.
© 2023 The Authors.
Figures
References
-
- WHO coronavirus (COVID-19) dashboard. World Health Organization. Accessed November 23, 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019
-
- Choi J.O., Shin D.H., Cho S.W., et al. Effect of preload on left ventricular longitudinal strain by 2D speckle tracking. Echocardiography. 2008;25(8):873–879. - PubMed