

Predicting Union, Osteomyelitis, and Amputation Outcomes of Gustilo IIIC Open Tibial Fractures: A Retrospective Study
- PMID: 38014457
- PMCID: PMC10782230
- DOI: 10.1111/os.13940
Predicting Union, Osteomyelitis, and Amputation Outcomes of Gustilo IIIC Open Tibial Fractures: A Retrospective Study
Abstract
Objective: Open tibial fractures are frequently encountered in high-energy traumas and can result in significant complications such as nonunion, osteomyelitis, and even amputation. Among open tibial fractures, Gustilo type IIIC cases are particularly challenging due to the concomitant occurrence of neurovascular injuries and soft tissue defects. This study aimed to assess factors that affect union time and complications in Gustilo IIIC tibial fractures.
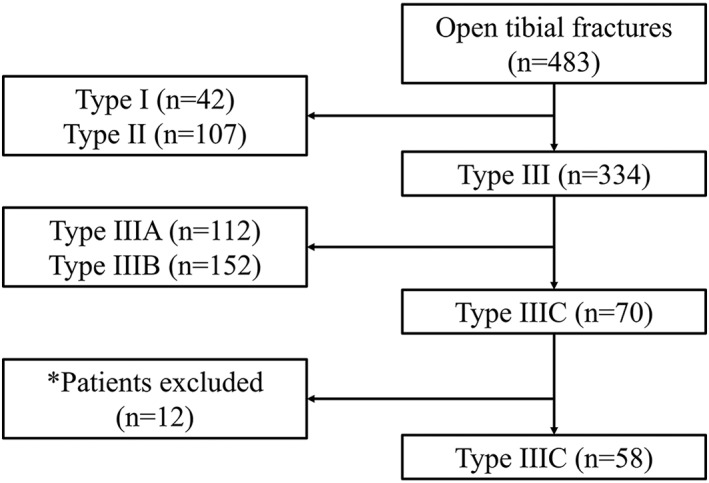
Methods: Patients who presented at our center with IIIC open tibial fractures from January 2000 to October 2020 were eligible for this retrospective analysis. Patient demographics, fracture characteristics, and the timing, number, and type of surgical intervention were documented. Outcomes of interest included union time, occurrence of osteomyelitis, and amputation. We performed univariate analyses including chi-squared test, Fischer's exact test, analysis of variance, and Kruskal-Wallis test based on the normality of the data and multivariate analyses including Cox proportional hazards model and logistic regression analyses.
Results: Fifty-eight patients were enrolled and grouped by fracture healing time; eight had timely union (13.8%); 27 had late union (46.6%); eight had delayed union (13.8%); three had nonunion (5.2%); and 12 underwent amputation (20.7%). Nine fractures (15.5%) were complicated by osteomyelitis. Union time was prolonged in cases of triple arterial injury, distal third fractures, multiple trauma with injury severity score (ISS) ≥ 16 points, and increased bone defect length. Additionally, a bone gap >50 mm, diabetes mellitus, low body mass index, and triple arterial injury in the lower leg were significant risk factors for amputation. A time from injury to definitive soft tissue coverage of more than 22 days was the major risk factor for osteomyelitis. A scoring system to predict union time was devised and the predicted probability of union within 2 years was stratified based on this score.
Conclusion: IIIC tibial fractures involving the distal third of the tibia, fractures with bone defects, triple arterial injury, and multiple trauma with ISS ≥16 points demonstrated delayed union, and an effective prediction system for union time was introduced in this study. Early soft tissue coverage can reduce the risk of osteomyelitis. Finally, diabetes and severe bone and soft tissue defects pose a higher risk of amputation.
Keywords: Gustilo IIIC tibial fractures; Injury severity score; Nonunion; Osteomyelitis; Union time.
© 2023 The Authors. Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare that there is no conflict of interest regarding the publication of this paper. No funding was provided for this study.
Figures



Similar articles
-
[Muscle flap transfer of the treatment of infected tibial and malleolar fractures and chronic osteomyelitis of the tibia].Acta Chir Orthop Traumatol Cech. 2007 Jun;74(3):162-70. Acta Chir Orthop Traumatol Cech. 2007. PMID: 17623603 Czech.
-
Individual risk factors for deep infection and compromised fracture healing after intramedullary nailing of tibial shaft fractures: a single centre experience of 480 patients.Injury. 2015 Apr;46(4):740-5. doi: 10.1016/j.injury.2014.12.018. Epub 2014 Dec 27. Injury. 2015. PMID: 25583638
-
The Effects of Timing of Soft Tissue Coverage on Outcomes After Reconstruction of Type IIIB Open Tibia Fractures.Orthopedics. 2019 Sep 1;42(5):260-266. doi: 10.3928/01477447-20190723-01. Epub 2019 Jul 29. Orthopedics. 2019. PMID: 31355903
-
Systematic review of patient reported outcomes from open tibia fractures in low and middle income countries.Injury. 2020 Feb;51(2):142-146. doi: 10.1016/j.injury.2019.11.015. Epub 2019 Nov 11. Injury. 2020. PMID: 31767370
-
Comparing outcomes following direct admission and early transfer to specialized trauma centers in open tibial fracture treatment: a systematic review and meta-analysis.Eur J Trauma Emerg Surg. 2024 Apr;50(2):467-476. doi: 10.1007/s00068-023-02366-x. Epub 2023 Sep 30. Eur J Trauma Emerg Surg. 2024. PMID: 37776341 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
