

Critical Care Management of Patients After Cardiac Arrest: A Scientific Statement From the American Heart Association and Neurocritical Care Society
- PMID: 38014539
- PMCID: PMC10775969
- DOI: 10.1161/CIR.0000000000001163
Critical Care Management of Patients After Cardiac Arrest: A Scientific Statement From the American Heart Association and Neurocritical Care Society
Abstract
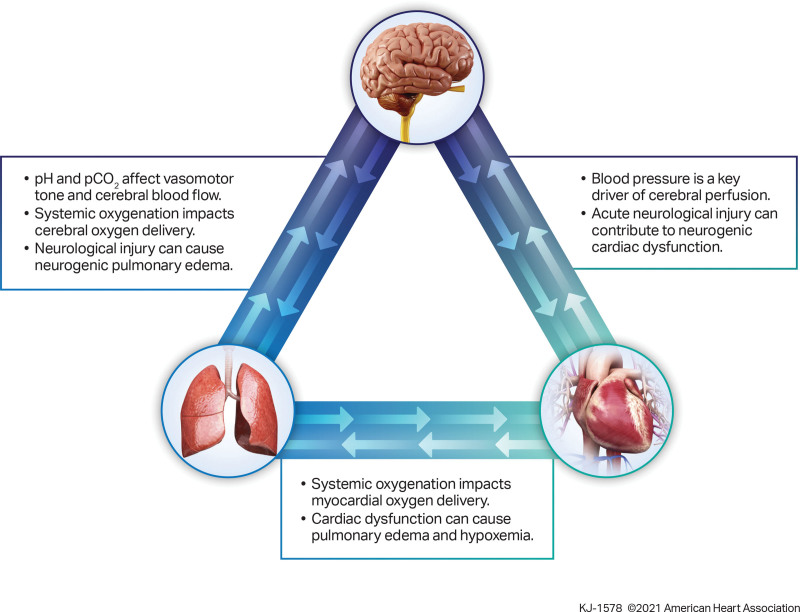
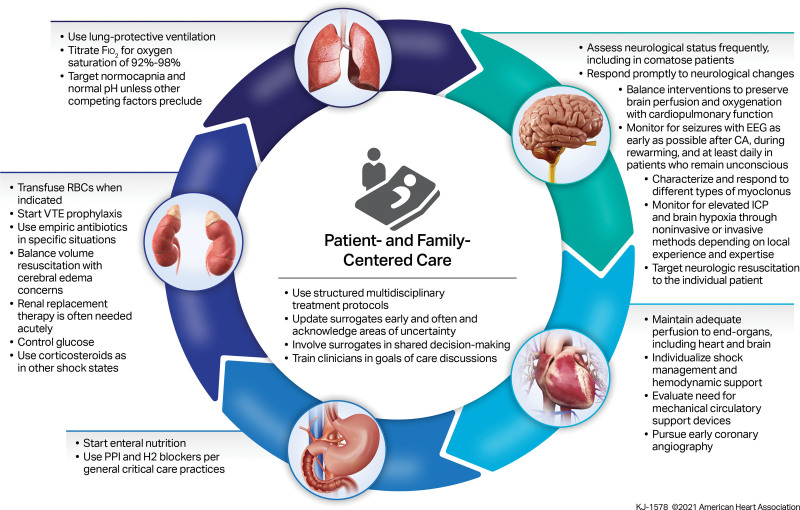
The critical care management of patients after cardiac arrest is burdened by a lack of high-quality clinical studies and the resultant lack of high-certainty evidence. This results in limited practice guideline recommendations, which may lead to uncertainty and variability in management. Critical care management is crucial in patients after cardiac arrest and affects outcome. Although guidelines address some relevant topics (including temperature control and neurological prognostication of comatose survivors, 2 topics for which there are more robust clinical studies), many important subject areas have limited or nonexistent clinical studies, leading to the absence of guidelines or low-certainty evidence. The American Heart Association Emergency Cardiovascular Care Committee and the Neurocritical Care Society collaborated to address this gap by organizing an expert consensus panel and conference. Twenty-four experienced practitioners (including physicians, nurses, pharmacists, and a respiratory therapist) from multiple medical specialties, levels, institutions, and countries made up the panel. Topics were identified and prioritized by the panel and arranged by organ system to facilitate discussion, debate, and consensus building. Statements related to postarrest management were generated, and 80% agreement was required to approve a statement. Voting was anonymous and web based. Topics addressed include neurological, cardiac, pulmonary, hematological, infectious, gastrointestinal, endocrine, and general critical care management. Areas of uncertainty, areas for which no consensus was reached, and future research directions are also included. Until high-quality studies that inform practice guidelines in these areas are available, the expert panel consensus statements that are provided can advise clinicians on the critical care management of patients after cardiac arrest.
Keywords: AHA Scientific Statements; critical care; heart arrest; hypoxia-ischemia, brain; resuscitation; shock, cardiogenic.
Conflict of interest statement
The American Heart Association and the Neurocritical Care Society make every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
Figures
References
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, et al. ; on behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141:e139–e596. doi: 10.1161/CIR.0000000000000757 - PubMed
-
- Kiguchi T, Okubo M, Nishiyama C, Maconochie I, Ong MEH, Kern KB, Wyckoff MH, McNally B, Christensen EF, Tjelmeland I, et al. Out-of-hospital cardiac arrest across the world: first report from the International Liaison Committee on Resuscitation (ILCOR). Resuscitation. 2020;152:39–49. doi: 10.1016/j.resuscitation.2020.02.044 - PubMed
-
- Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore-Mensah Y, et al. ; on behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2022 update: a report from the American Heart Association [published correction appears in Circulation. 2022;146:e141]. Circulation. 2022;145:e153–e639. doi: 10.1161/CIR.0000000000001052 - PubMed
-
- Girotra S, Nallamothu BK, Tang Y, Chan PS; American Heart Association Get With The Guidelines–Resuscitation Investigators. Association of hospital-level acute resuscitation and postresuscitation survival with overall risk-standardized survival to discharge for in-hospital cardiac arrest. JAMA Netw Open. 2020;3:e2010403. doi: 10.1001/jamanetworkopen.2020.10403 - PMC - PubMed
-
- Panchal AR, Bartos JA, Cabañas JG, Donnino MW, Drennan IR, Hirsch KG, Kudenchuk PJ, Kurz MC, Lavonas EJ, Morley PT, et al. ; on behalf of the Adult Basic and Advanced Life Support Writing Group. Part 3: adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142(suppl 2):S366–S468. doi: 10.1161/CIR.0000000000000916 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
