

Omics and Extreme Phenotyping Reveal Longitudinal Association Between Left Atrial Size and Pulmonary Vascular Resistance in Group 2 Pulmonary Hypertension
- PMID: 38014658
- PMCID: PMC10727316
- DOI: 10.1161/JAHA.123.031746
Omics and Extreme Phenotyping Reveal Longitudinal Association Between Left Atrial Size and Pulmonary Vascular Resistance in Group 2 Pulmonary Hypertension
Abstract
Background: Left heart disease is the most common cause of pulmonary hypertension (PH) and is frequently accompanied by increases in pulmonary vascular resistance. However, the distinction between phenotypes of PH due to left heart disease with a normal or elevated pulmonary vascular resistance-isolated postcapillary PH (IpcPH) and combined pre- and postcapillary PH (CpcPH), respectively-has been incompletely defined using unbiased methods.
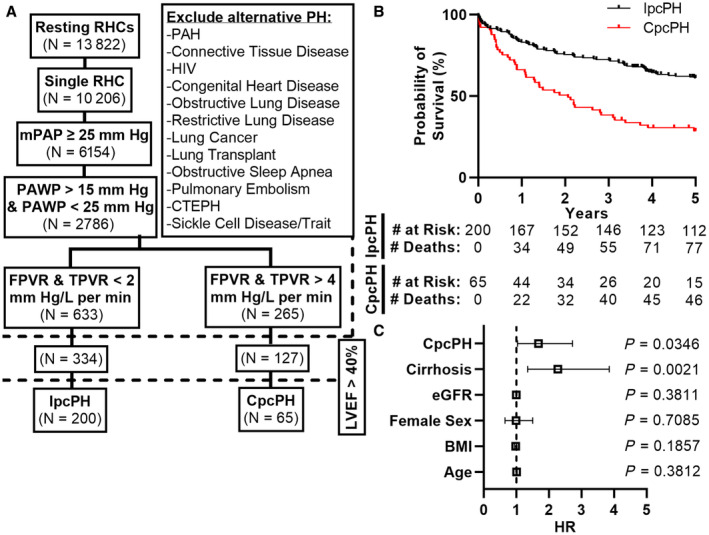
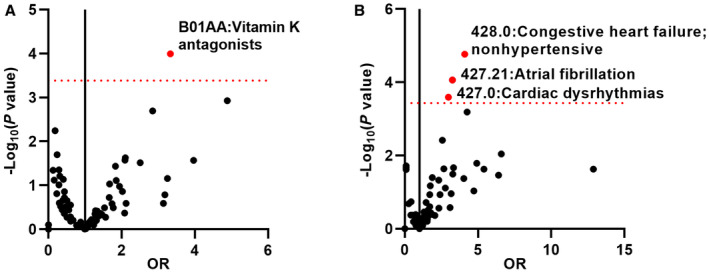
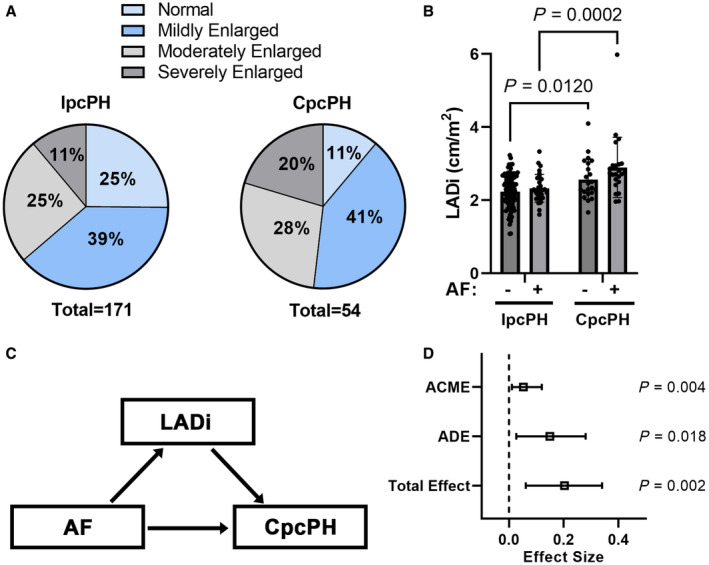
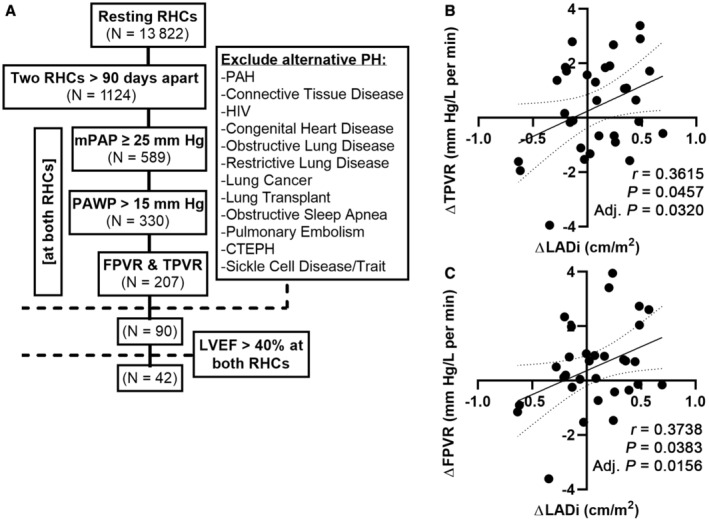
Methods and results: Patients with extremes of IpcPH versus CpcPH were identified from a single-center record of those who underwent right heart catheterization. Individuals with left ventricular ejection fraction <40% or with potential causes of PH beyond left heart disease were excluded. Medication usage in IpcPH and CpcPH was compared across Anatomical Therapeutic Chemical classes and identified vitamin K antagonists as the only medication with pharmacome-wide significance, being more commonly used in CpcPH and for an indication of atrial fibrillation in ≈90% of instances. Accordingly, atrial fibrillation prevalence was significantly higher in CpcPH in a phenome-wide analysis. Review of echocardiographic data most proximal to right heart catheterization revealed that left atrial diameter indexed to body surface area-known to be associated with atrial fibrillation-was increased in CpcPH regardless of the presence of atrial fibrillation. An independent cohort with serial right heart catheterizations and PH-left heart disease showed a significant positive correlation between change in left atrial diameter indexed to body surface area and change in pulmonary vascular resistance.
Conclusions: Guided by pharmacomic and phenomic screens in a rigorously phenotyped cohort, we identify a longitudinal association between left atrial diameter indexed to body surface area and pulmonary vascular resistance with implications for the future development of diagnostic, prognostic, and therapeutic tools.
Keywords: atrial fibrillation; left atrium; pulmonary hypertension; pulmonary vascular resistance.
Figures
References
-
- Wijeratne DT, Lajkosz K, Brogly SB, Lougheed MD, Jiang L, Housin A, Barber D, Johnson A, Doliszny KM, Archer SL. Increasing incidence and prevalence of World Health Organization groups 1 to 4 pulmonary hypertension: a population‐based cohort study in Ontario, Canada. Circ Cardiovasc Qual Outcomes. 2018;11:e003973. doi: 10.1161/CIRCOUTCOMES.117.003973 - DOI - PMC - PubMed
-
- Palazzini M, Dardi F, Manes A, Bacchi Reggiani ML, Gotti E, Rinaldi A, Albini A, Monti E, Galie N. Pulmonary hypertension due to left heart disease: analysis of survival according to the haemodynamic classification of the 2015 ESC/ERS guidelines and insights for future changes. Eur J Heart Fail. 2018;20:248–255. doi: 10.1002/ejhf.860 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
