

Telemedical Monitoring of Plantar Temperature in Diabetic Patients at Risk of Foot Ulcers
- PMID: 38015655
- PMCID: PMC10916763
- DOI: 10.3238/arztebl.m2023.0229
Telemedical Monitoring of Plantar Temperature in Diabetic Patients at Risk of Foot Ulcers
Abstract
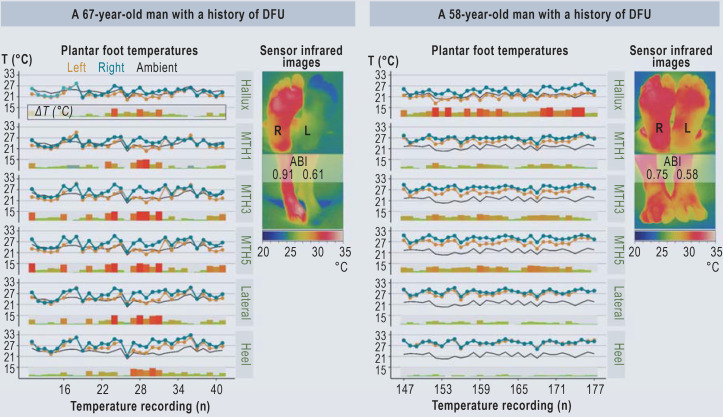
Background: The worldwide prevalence of diabetic foot ulcers (DFUs) among persons with diabetes is estimated at 6.3%, with an annual incidence of 9.1 to 26.1 million persons. The early detection of asymmetrical plantar temperature elevation, followed by reduction of weight-bearing on the affected foot, may be an effective mode of prevention.
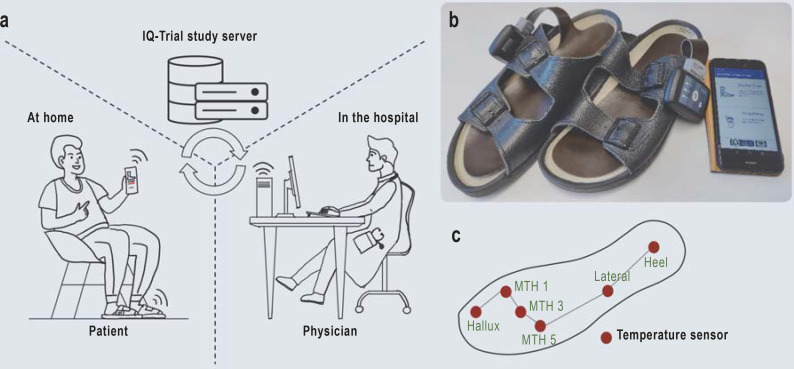
Methods: Patients with diabetes and peripheral neuropathy (DFU risk groups 2/3) were monitored for plantar abnormalities with a telemedical system consisting of sole inserts with temperature sensors and photographic documentation. An open, prospective, randomized controlled trial was performed to determine whether this system prevented DFUs. The intervention and control groups were also trained in ulcer prevention and observed in follow-up at 6-month intervals for 24 months.
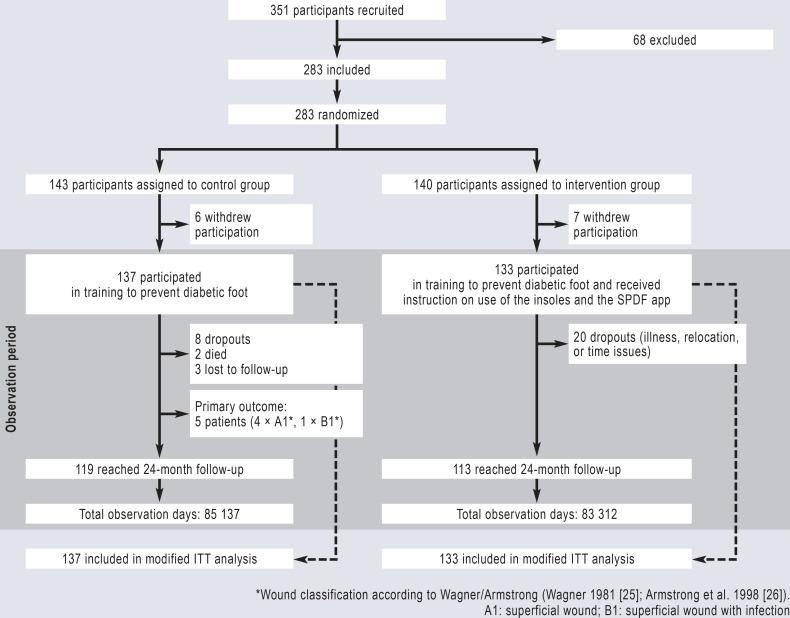
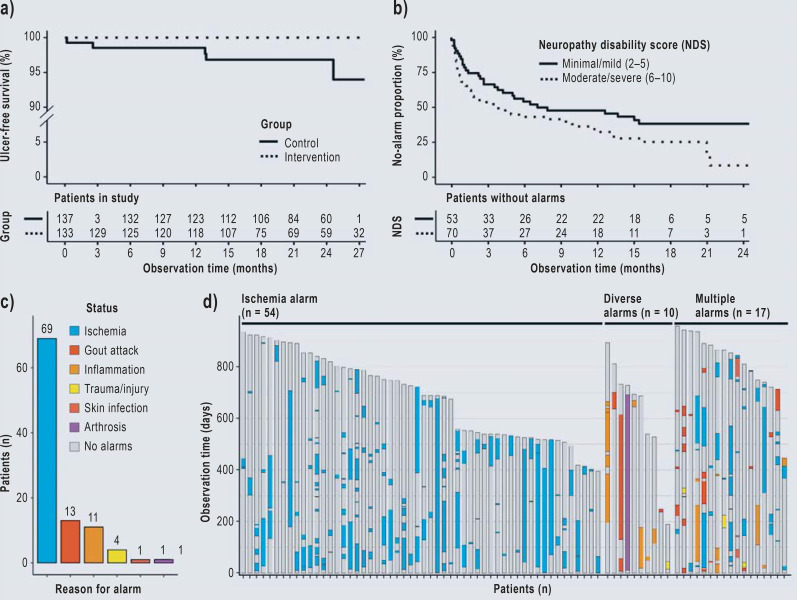
Results: 283 patients were recruited. In 85 137 observation days, DFUs arose in five patients in the control group (n = 143) and in no patient in the intervention group (n = 140). The primary outcome measure was the hazard ratio, which was calculated to be 0.015 (95% confidence interval [0; 19,717]; p = 0.25) after adjustment for age, sex, severity of neuropathy, and risk class. There were 239 alarms and 75 instructions to reduce weight-bearing on the foot. The subjects carried out the telemedical application on about 70% of the days of observation. Quality of life improved in both groups.
Conclusion: The tele-health system used in this trial is practical and enables the early detection of morbidity. Likely explanations for the unexpectedly low ulceration rate in this trial (and, in turn, for the lack of statistical significance) include the availability of a training program and regular follow-up examinations to patients in both arms of the trial, along with lower mobility levels due to the COVID pandemic.
Figures
Similar articles
-
Study protocol for a randomized controlled trial to test for preventive effects of diabetic foot ulceration by telemedicine that includes sensor-equipped insoles combined with photo documentation.Trials. 2019 Aug 22;20(1):521. doi: 10.1186/s13063-019-3623-x. Trials. 2019. PMID: 31439007 Free PMC article.
-
Innovative intelligent insole system reduces diabetic foot ulcer recurrence at plantar sites: a prospective, randomised, proof-of-concept study.Lancet Digit Health. 2019 Oct;1(6):e308-e318. doi: 10.1016/S2589-7500(19)30128-1. Epub 2019 Sep 26. Lancet Digit Health. 2019. PMID: 33323253 Clinical Trial.
-
Effects of novel diabetic therapeutic footwear on preventing ulcer recurrence in patients with a history of diabetic foot ulceration: study protocol for an open-label, randomized, controlled trial.Trials. 2021 Feb 17;22(1):151. doi: 10.1186/s13063-021-05098-8. Trials. 2021. PMID: 33597005 Free PMC article.
-
The role of foot pressure measurement in the prediction and prevention of diabetic foot ulceration-A comprehensive review.Diabetes Metab Res Rev. 2020 May;36(4):e3258. doi: 10.1002/dmrr.3258. Epub 2019 Dec 11. Diabetes Metab Res Rev. 2020. PMID: 31825163 Free PMC article. Review.
-
Diabetic Foot Ulcers and Cardiac Autonomic Neuropathy.Clin Ther. 2022 Feb;44(2):323-330. doi: 10.1016/j.clinthera.2021.12.002. Epub 2021 Dec 30. Clin Ther. 2022. PMID: 34974945 Review.
Cited by
-
Peripheral Arterial Disease and the Diabetic Foot Syndrome: Neuropathy Makes the Difference! A Narrative Review.J Clin Med. 2024 Apr 8;13(7):2141. doi: 10.3390/jcm13072141. J Clin Med. 2024. PMID: 38610906 Free PMC article. Review.
-
Video game-based application for fall risk assessment: a proof-of-concept cohort study.EClinicalMedicine. 2024 Nov 27;78:102947. doi: 10.1016/j.eclinm.2024.102947. eCollection 2024 Dec. EClinicalMedicine. 2024. PMID: 39677357 Free PMC article.
References
-
- Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376:2367–2375. - PubMed
-
- Grennan D. Diabetic foot ulcers. JAMA. 2019;321 - PubMed
-
- Zhang P, Lu J, Jing Y, Tang S, Zhu D, Bi Y. Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis. Ann Med. 2017;49:106–116. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical