

Revolutionizing sphincter preservation in ultra-low rectal cancer: exploring the potential of transanal endoscopic intersphincteric resection (taE-ISR): a propensity score-matched cohort study
- PMID: 38016136
- PMCID: PMC10871607
- DOI: 10.1097/JS9.0000000000000945
Revolutionizing sphincter preservation in ultra-low rectal cancer: exploring the potential of transanal endoscopic intersphincteric resection (taE-ISR): a propensity score-matched cohort study
Abstract
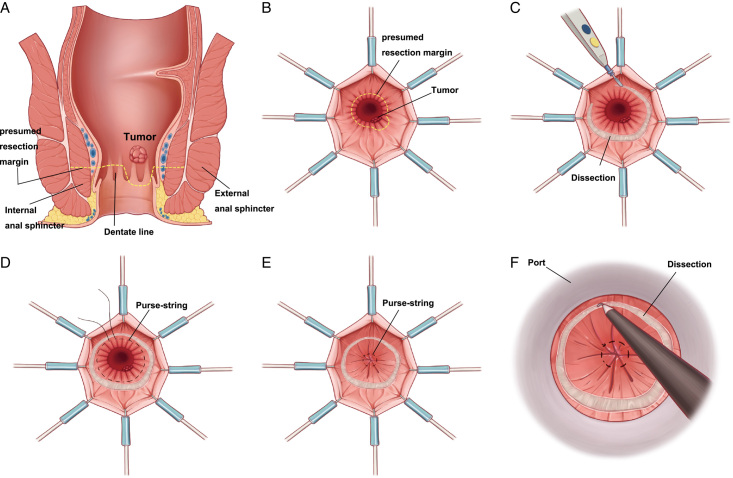
Background: With the optimization of neoadjuvant treatment regimens, the indications for intersphincteric resection (ISR) have expanded. However, limitations such as unclear surgical field, impaired anal function, and failure of anal preservation still exist. Transanal total mesorectal excision can complement the drawbacks of ISR. Therefore, this study combined these two techniques and proposed transanal endoscopic intersphincteric resection (taE-ISR), aiming to explore the value of this novel technique in anal preservation for ultra-low rectal cancer.
Material and methods: Four high-volume centres were involved. After 1:1 propensity score-matching, patients with ultra-low rectal cancer underwent taE-ISR ( n =90) or ISR ( n =90) were included. Baseline characteristics, perioperative outcomes, pathological results, and follow-up were compared between the two groups. A nomogram model was established to assess the potential risks of anal preservation.
Results: The incidence of adjacent organ injury (0.0% vs. 5.6%, P =0.059), positive distal resection margin (1.1% vs. 8.9%, P =0.034), and incomplete specimen (2.2% vs. 13.3%, P =0.012) were lower in taE-ISR group. Moreover, the anal preservation rate was significantly higher in taE-ISR group (97.8% vs. 82.2%, P =0.001). Patients in the taE-ISR group showed a better disease-free survival ( P =0.044) and lower cumulative recurrence ( P =0.022) compared to the ISR group. Surgery procedure, tumour distance, and adjacent organ injury were factors influencing anal preservation in patients with ultra-low rectal cancer.
Conclusion: taE-ISR technique was safe, feasible, and improved surgical quality, anal preservation rate and survival outcomes in ultra-low rectal cancer patients. It held significant clinical value and showed promising application prospects for anal preservation.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare that there is no conflict of interest regarding the publication of this paper.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures





Similar articles
-
Short-term outcomes of transanal endoscopic intersphincteric resection for locally advanced rectal cancer after neoadjuvant chemoradiotherapy: A single-center retrospective cohort study.Eur J Surg Oncol. 2025 Jul;51(7):109984. doi: 10.1016/j.ejso.2025.109984. Epub 2025 Mar 21. Eur J Surg Oncol. 2025. PMID: 40203672
-
Long-term efficacy and short-term outcomes of intersphincteric resection vs abdominoperineal resection in patients with ultra-low rectal cancer.World J Gastroenterol. 2025 Aug 7;31(29):110004. doi: 10.3748/wjg.v31.i29.110004. World J Gastroenterol. 2025. PMID: 40809926 Free PMC article.
-
Oncological Outcomes of Intersphincteric Resection Versus Abdominoperineal Resection for ypT3 Low Rectal Cancer After Neoadjuvant Chemoradiotherapy: A Multicenter Retrospective Analysis.Dis Colon Rectum. 2025 Aug 1;68(8):951-961. doi: 10.1097/DCR.0000000000003821. Epub 2025 May 7. Dis Colon Rectum. 2025. PMID: 40331664
-
The impact of transanal local excision of early rectal cancer on completion rectal resection without neoadjuvant chemoradiotherapy: a systematic review.Tech Coloproctol. 2021 Sep;25(9):997-1010. doi: 10.1007/s10151-020-02401-8. Epub 2021 Jun 25. Tech Coloproctol. 2021. PMID: 34173121
-
Systematic review of outcomes after intersphincteric resection for low rectal cancer.Br J Surg. 2012 May;99(5):603-12. doi: 10.1002/bjs.8677. Epub 2012 Jan 13. Br J Surg. 2012. PMID: 22246846
Cited by
-
The Review of Modified Intersphincteric Resection in the Treatment of Ultra-Low Rectal Cancer.Curr Treat Options Oncol. 2025 Feb;26(2):84-91. doi: 10.1007/s11864-025-01291-y. Epub 2025 Jan 23. Curr Treat Options Oncol. 2025. PMID: 39847237 Free PMC article. Review.
-
Comparison of laparoscopic versus robot-assisted sugery for rectal cancer after neo-adjuvant therapy: a large volume single center experience.BMC Surg. 2025 Mar 12;25(1):98. doi: 10.1186/s12893-025-02764-5. BMC Surg. 2025. PMID: 40075413 Free PMC article.
References
-
- Schiessel R, Karner-Hanusch J, Herbst F, et al. . Intersphincteric resection for low rectal tumours. Br J Surg 1994;81:1376–1378. - PubMed
-
- André T, Shiu KK, Kim TW, et al. . Pembrolizumab in microsatellite-instability-high advanced colorectal cancer. N Engl J Med 2020;383:2207–2218. - PubMed
-
- Conroy T, Bosset JF, Etienne PL, et al. . Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol 2021;22:702–715. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
