

Safety and effectiveness of totally laparoscopic total gastrectomy vs laparoscopic-assisted total gastrectomy: a meta-analysis
- PMID: 38016295
- PMCID: PMC10871622
- DOI: 10.1097/JS9.0000000000000921
Safety and effectiveness of totally laparoscopic total gastrectomy vs laparoscopic-assisted total gastrectomy: a meta-analysis
Abstract
Background: For gastric cancer with total gastrectomy, the usual laparoscopic surgical approaches are totally laparoscopic total gastrectomy (TLTG) and laparoscopic-assisted total gastrectomy (LATG). Due to its difficult anastomotic technique, the adoption of TLTG is limited. Therefore, surgeons prefer using LATG, which also led to TLTG being somewhat overlooked, so there is no clear conclusion today as to which surgical procedure is more favorable to the patient's recovery. This article aimed to compare the safety and short-term outcomes of the two surgical approaches.
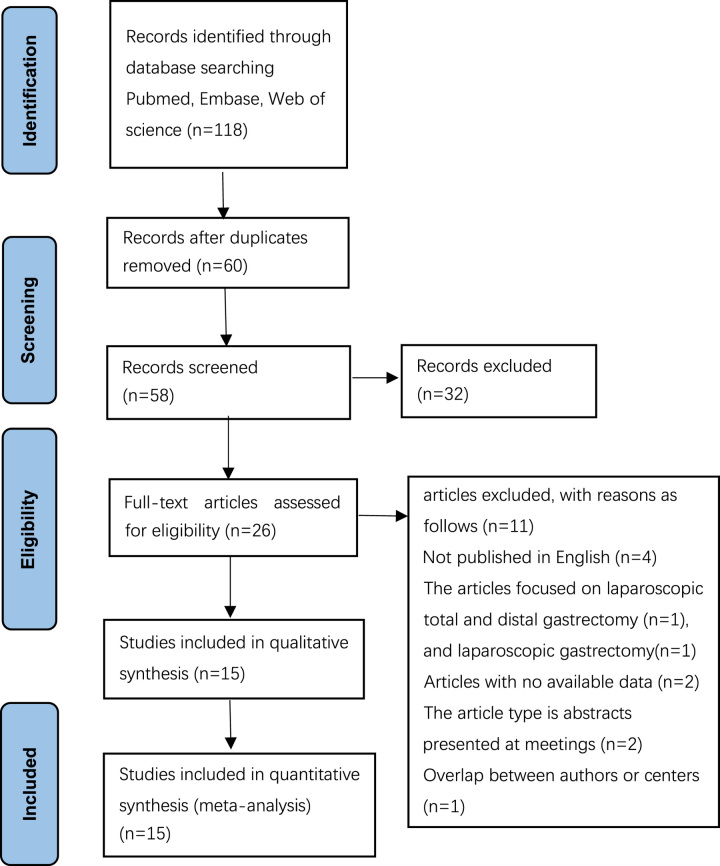
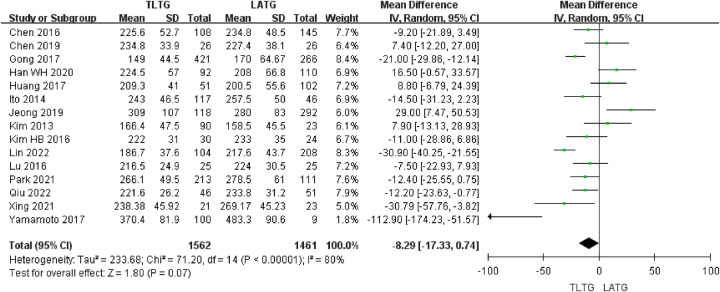
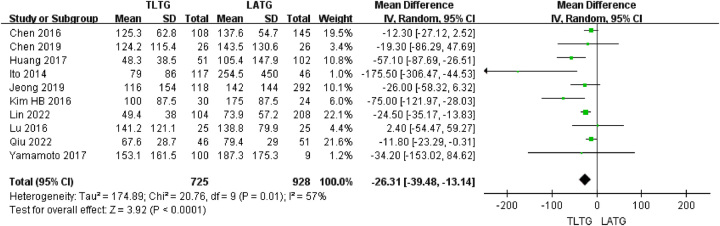
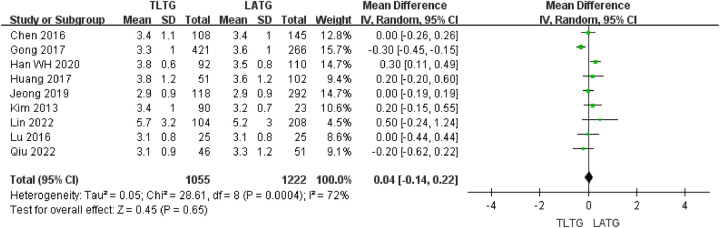
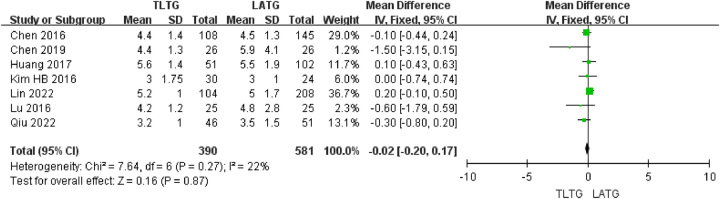
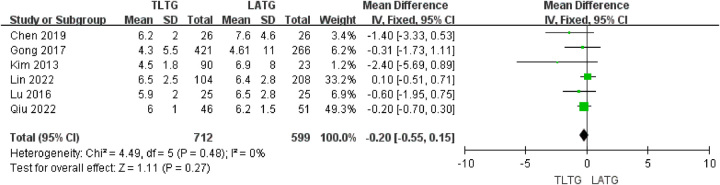
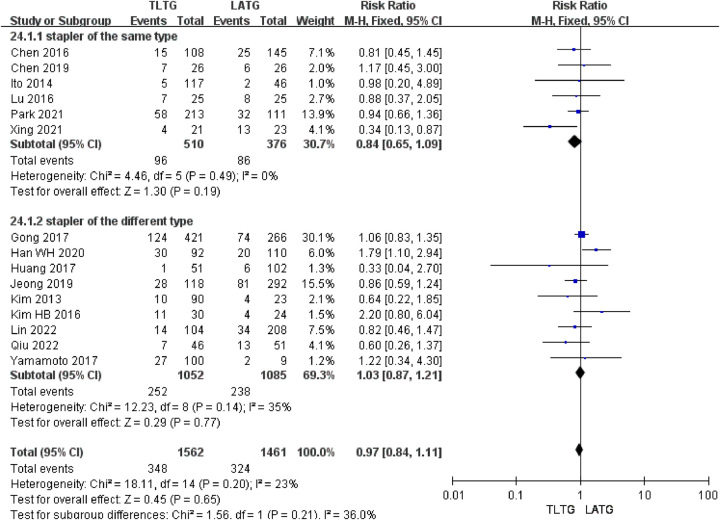
Materials and methods: Studies comparing TLTG and LATG, published up to December 2022, were searched in PubMed, Web of Science, and Embase databases. The study outcomes, including operative time, blood loss, anastomosis time, number of retrieved lymph nodes, proximal and distal resection margins, time to first fluid and soft diet, hospitalization duration, time to first flatus, and postsurgical and anastomotic complications, were compared between these two different surgical procedures. Statistics were analyzed with RevMan 5.4 and Stata 13.1.
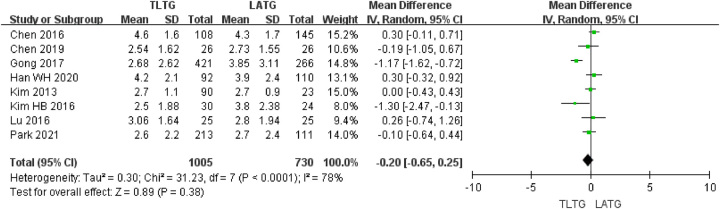
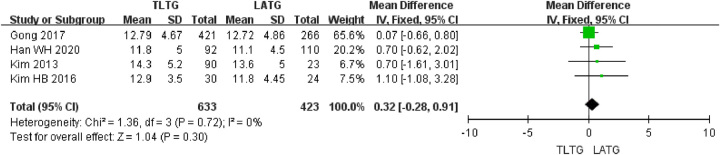
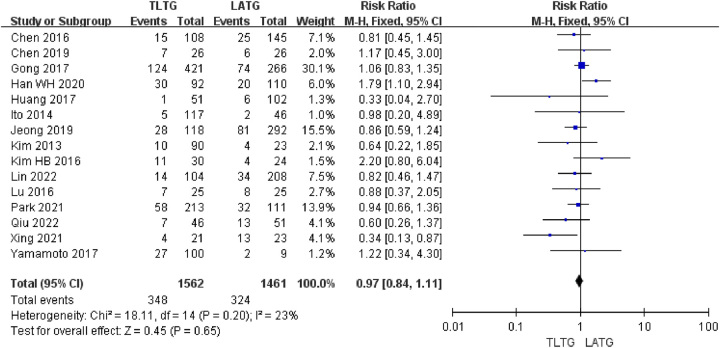
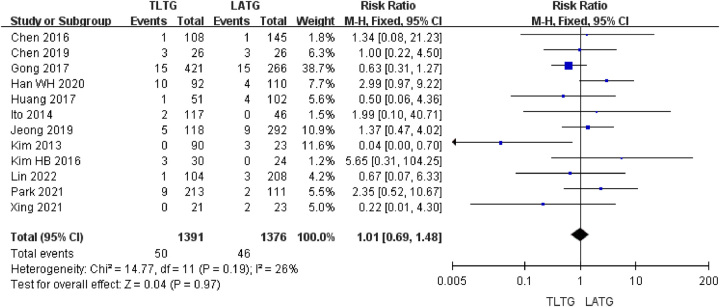
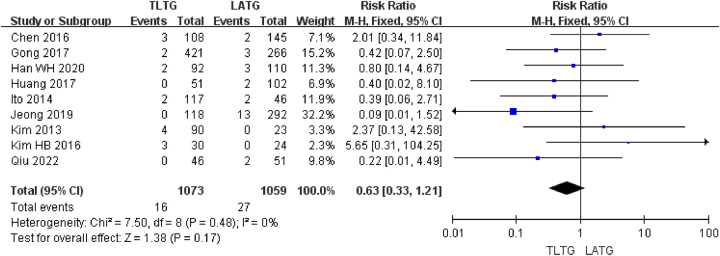
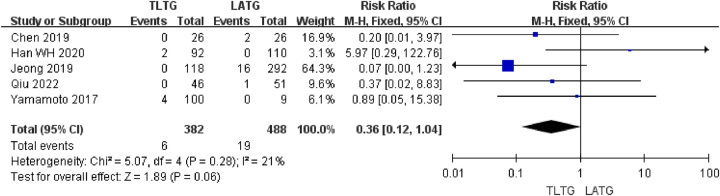
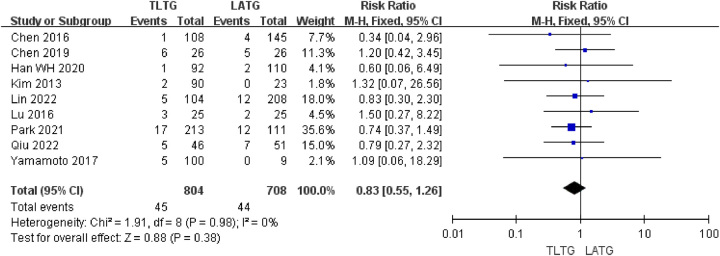
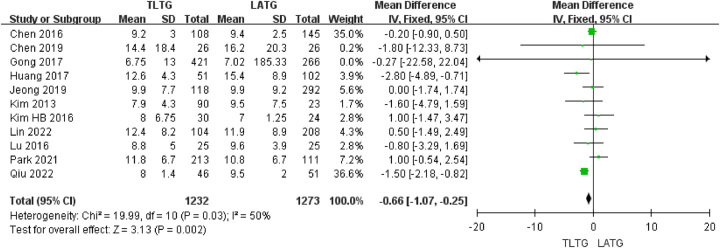
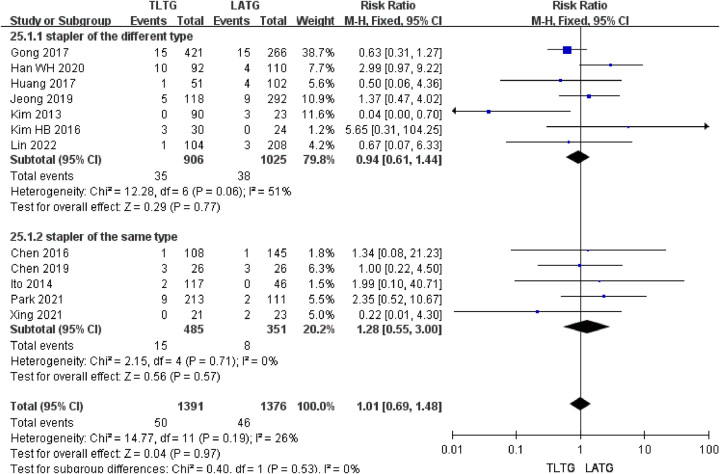
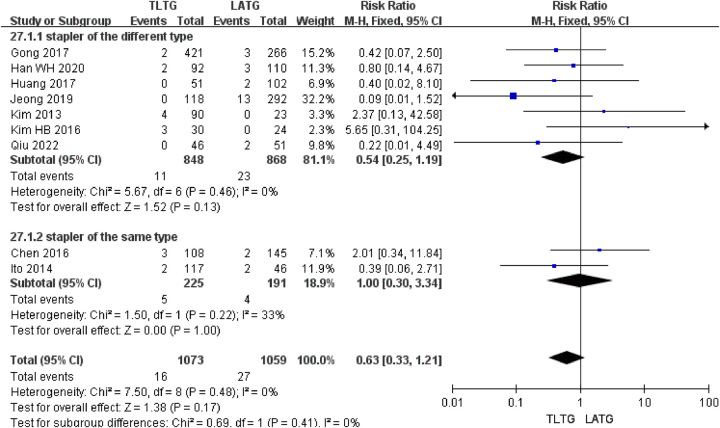
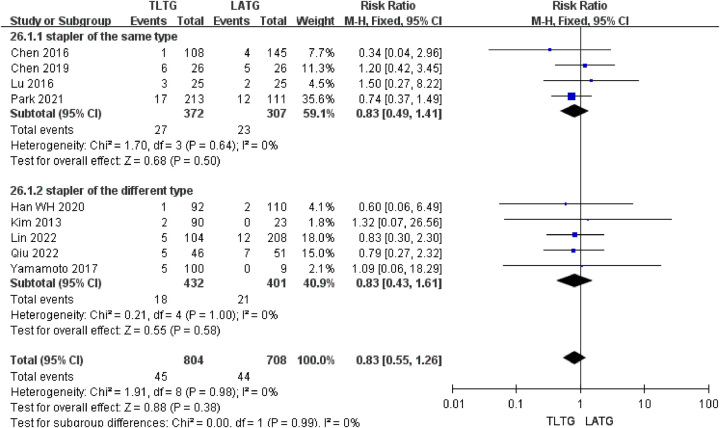
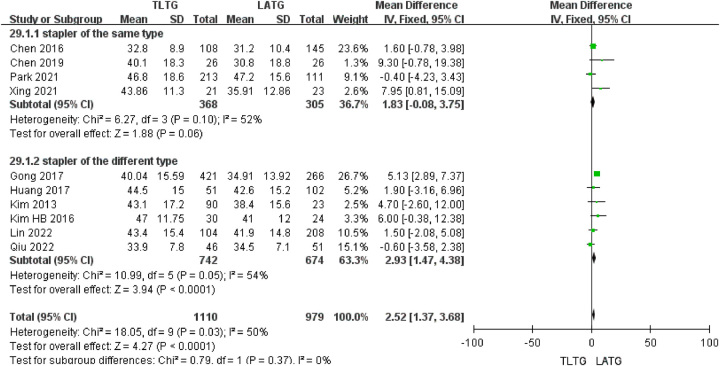
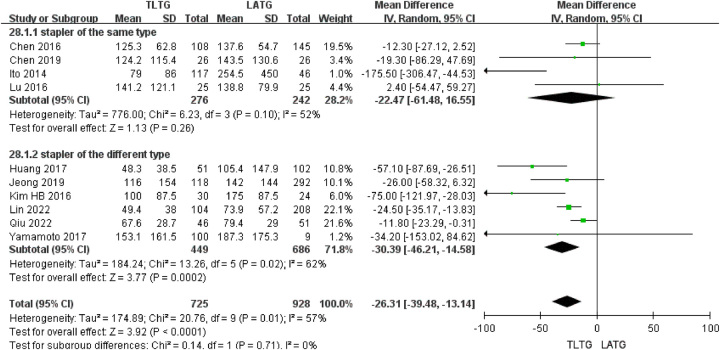
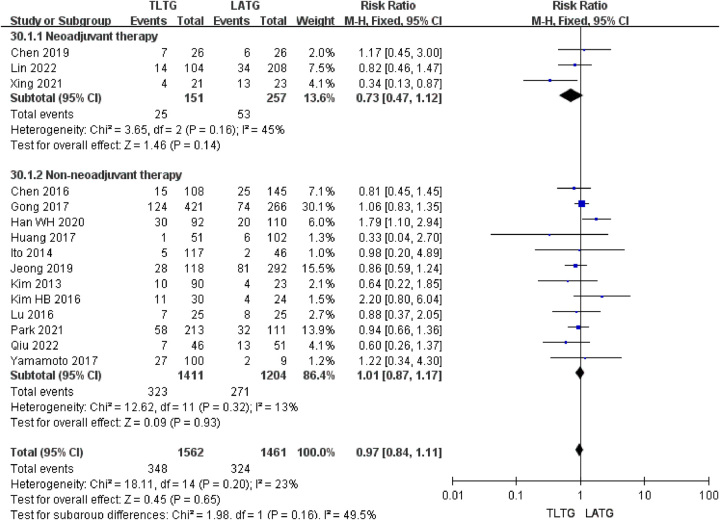
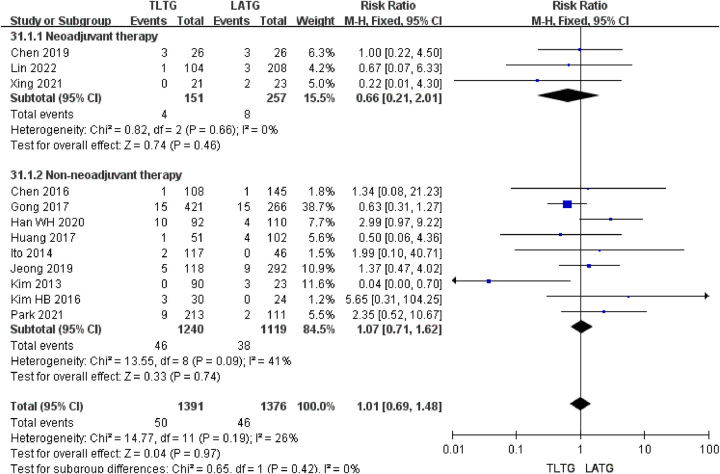
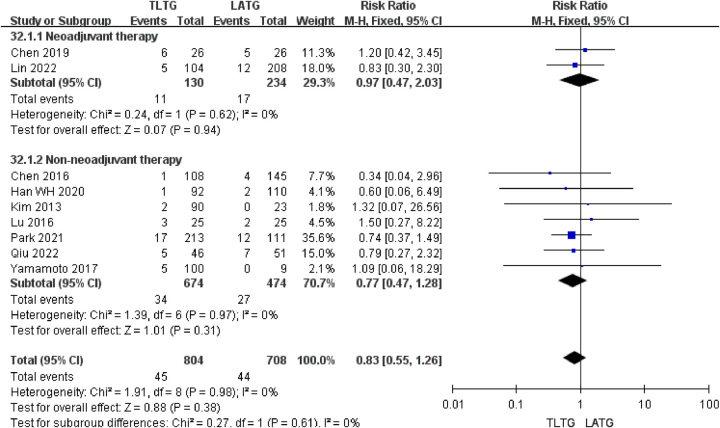
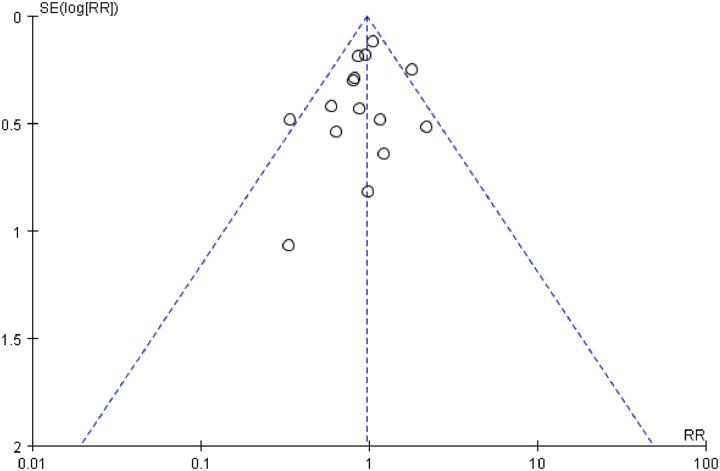
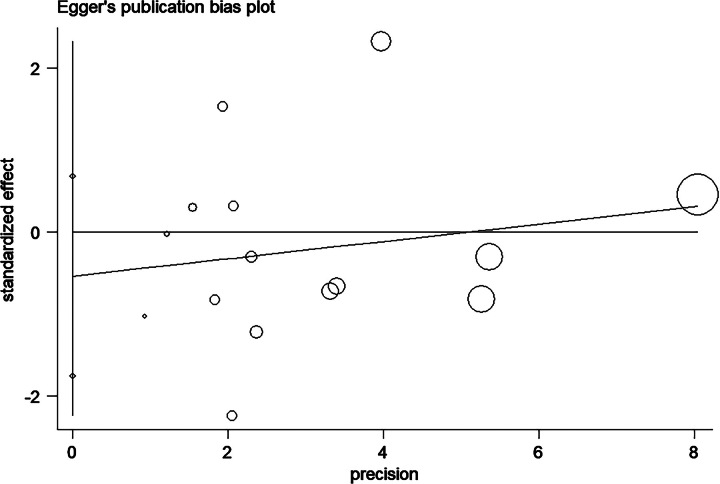
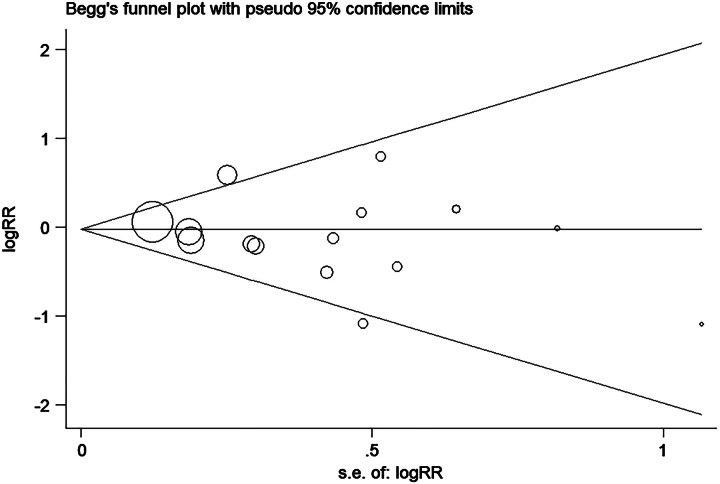
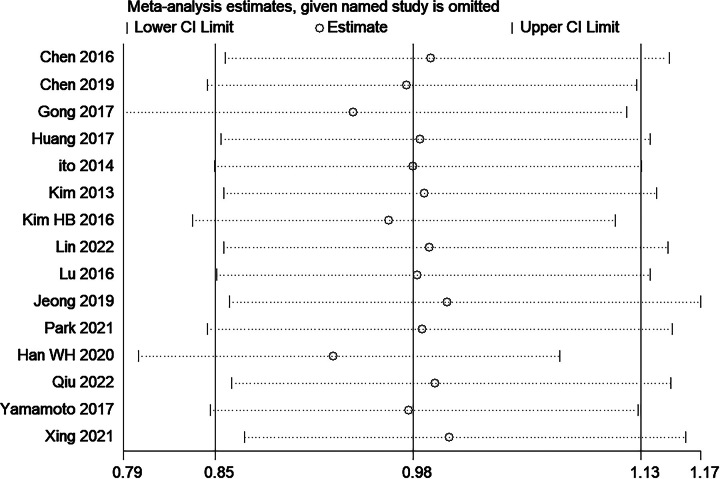
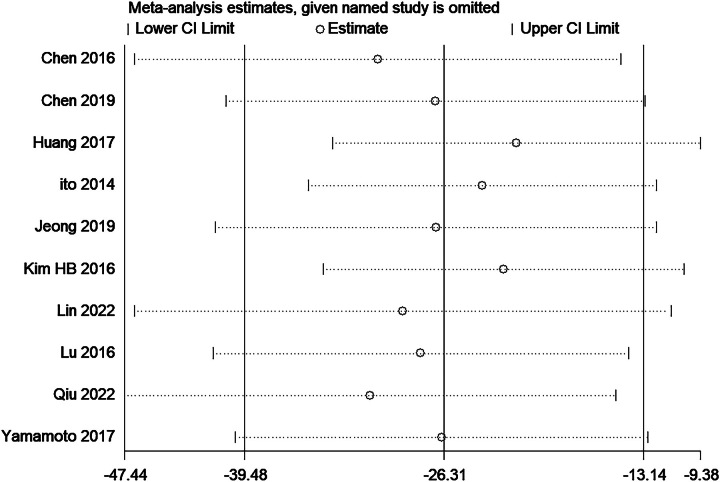
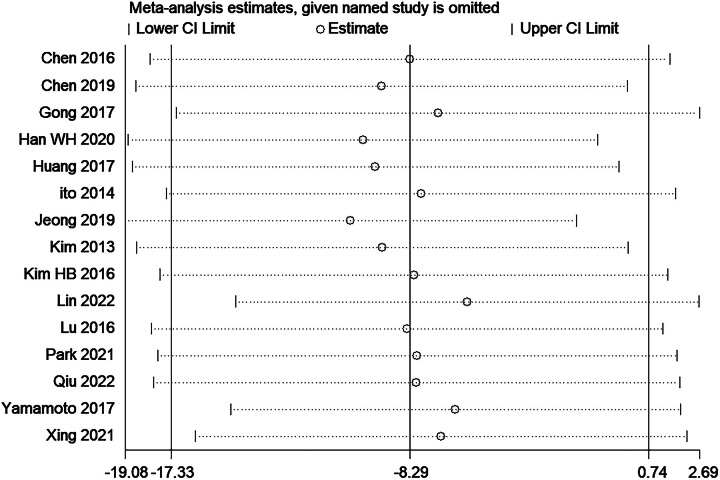
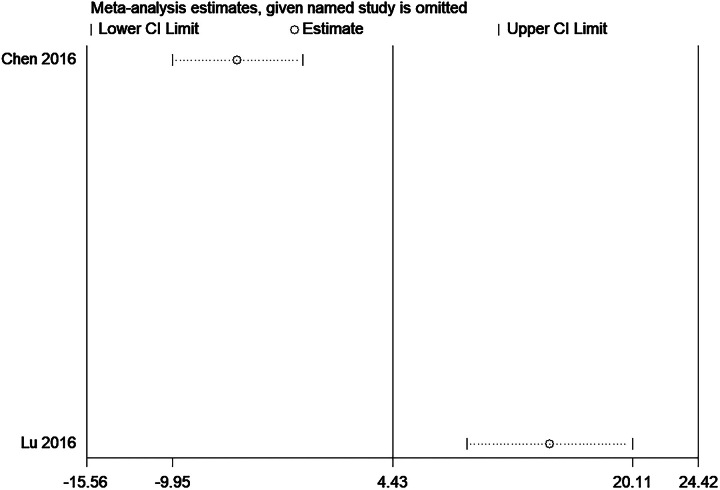
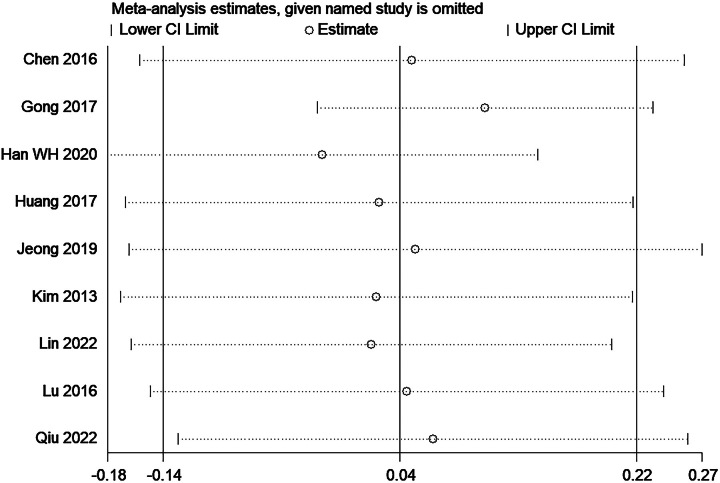
Results: Fifteen publications were included in this study. The total sample included 3023 cases. The meta-analysis revealed no significant difference in overall postoperative complications between the two surgical approaches ( P >0.05). Compared with LATG, TLTG led to reduced intraoperative blood loss ( P <0.0001), an increased number of lymphatic node dissections ( P <0.0001), and decreased hospitalization duration ( P =0.002). However, operative time, anastomosis time, pulmonary infection, resection margins, time to first fluid and soft diet, time to first flatus and anastomosis-related complications were no significant difference between TLTG and LATG groups ( P >0.05).
Conclusion: TLTG did not lead to an increase in overall postoperative complications, which is a reliable surgical approach for treatment of gastric cancer. Moreover, it may reduce harm to patients and enable them to obtain better surgical outcomes.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors promise that this research has no conflict of interest with any party.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures

References
-
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–249. - PubMed
-
- Johnston FM, Beckman M. Updates on management of gastric cancer. Curr Oncol Rep 2019;21:67. - PubMed
-
- Kitano S, Iso Y, Moriyama M, et al. Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc 1994;4:146–148. - PubMed
-
- van der Veen A, Brenkman HJF, Seesing MFJ, et al. Laparoscopic Versus Open Gastrectomy for Gastric Cancer (LOGICA): a multicenter randomized clinical trial. J Clin Oncol 2021;39:978–989. - PubMed
-
- Wang J, Wang JC, Song B, et al. Comparative study of laparoscopic-assisted and open total gastrectomy for Siewert Types II and III adenocarcinoma of the esophagogastric junction. J Cell Physiol 2019;234:11235–11239. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
