

High-dimensional single-cell proteomics analysis of esophageal squamous cell carcinoma reveals dynamic alterations of the tumor immune microenvironment after neoadjuvant therapy
- PMID: 38016720
- PMCID: PMC10685958
- DOI: 10.1136/jitc-2023-007847
High-dimensional single-cell proteomics analysis of esophageal squamous cell carcinoma reveals dynamic alterations of the tumor immune microenvironment after neoadjuvant therapy
Abstract
Background: Dynamic alterations of the tumor immune microenvironment in esophageal squamous cell carcinoma (ESCC) after different neoadjuvant therapies were understudied.
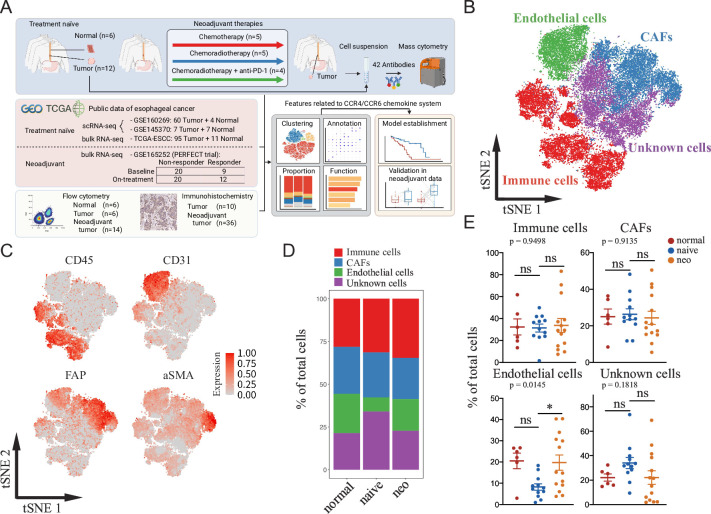
Methods: We used mass cytometry with a 42-antibody panel for 6 adjacent normal esophageal mucosa and 26 tumor samples (treatment-naïve, n=12; postneoadjuvant, n=14) from patients with ESCC. Single-cell RNA sequencing of previous studies and bulk RNA sequencing from The Cancer Genome Atlas were analyzed, flow cytometry, immunohistochemistry, and immunofluorescence analyses were performed.
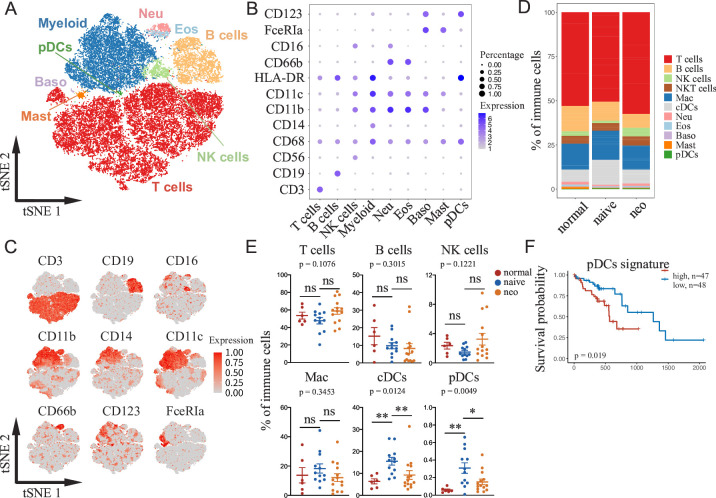
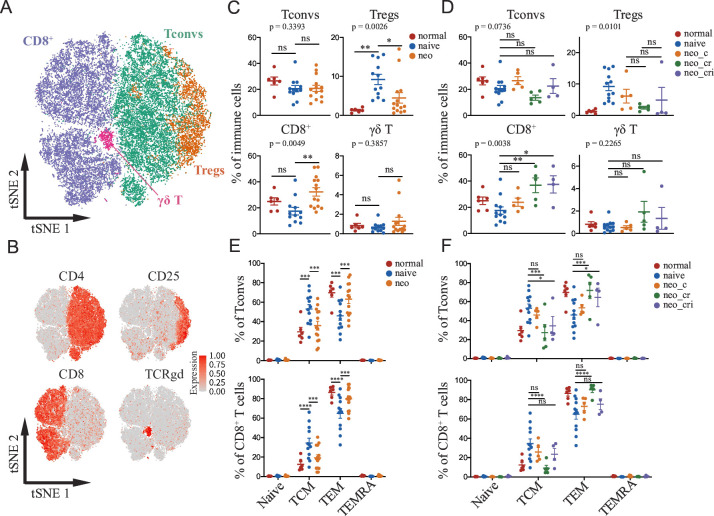
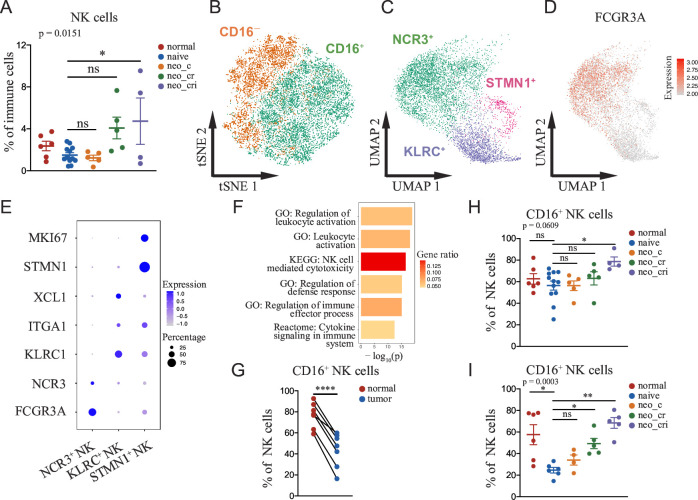
Results: Poor tumor regression was observed in the neoadjuvant chemotherapy group. Radiotherapy-based regimens enhanced CD8+ T cells but diminished regulatory T cells and promoted the ratio of effector memory to central memory T cells. Immune checkpoint blockade augmented NK cell activation and cytotoxicity by increasing the frequency of CD16+ NK cells. We discovered a novel CCR4+CCR6+ macrophage subset that correlated with the enrichment of corresponding chemokines (CCL3/CCL5/CCL17/CCL20/CCL22). We established a CCR4/CCR6 chemokine-based model that stratified ESCC patients with differential overall survival and responsiveness to neoadjuvant chemoradiotherapy combined with immunotherapy, which was validated in two independent cohorts of esophageal cancer with neoadjuvant treatment.
Conclusions: This work reveals that neoadjuvant therapy significantly regulates the cellular composition of the tumor immune microenvironment in ESCC and proposes a potential model of CCR4/CCR6 system to predict the benefits from neoadjuvant chemoradiotherapy combined with immunotherapy.
Keywords: Immune Checkpoint Inhibitors; Radiotherapy; Tumor Biomarkers; Tumor Microenvironment.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: HWMvL reports research funding and/or medication supply from Bristol-Myers Squibb, Bayer Schering Pharma, Celgene, Janssen-Cilag, Lilly, Nordic Pharma, Philips Healthcare, Roche, Merck Sharp and Dohme, Servier, Incyte, and consultant/advisory board members for Lilly, Nordic Pharma, Bristol-Myers Squibb, Dragonfly, Merck Sharp and Dohme, Servier, outside the submitted work. The remaining authors have declared no conflicts of interest.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials