

MET-receptor targeted fluorescent imaging and spectroscopy to detect multifocal papillary thyroid cancer
- PMID: 38017325
- PMCID: PMC11178647
- DOI: 10.1007/s00259-023-06525-5
MET-receptor targeted fluorescent imaging and spectroscopy to detect multifocal papillary thyroid cancer
Abstract
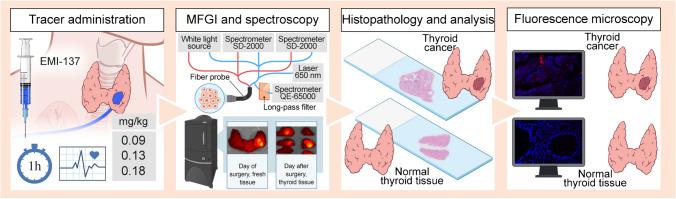
Purpose: Multifocal disease in PTC is associated with an increased recurrence rate. Multifocal disease (MD) is underdiagnosed with the current gold standard of pre-operative ultrasound staging. Here, we evaluate the use of EMI-137 targeted molecular fluorescence-guided imaging (MFGI) and spectroscopy as a tool for the intra-operative detection of uni- and multifocal papillary thyroid cancer (PTC) aiming to improve disease staging and treatment selection.
Methods: A phase-1 study (NCT03470259) with EMI-137 was conducted to evaluate the possibility of detecting PTC using MFGI and quantitative fiber-optic spectroscopy.
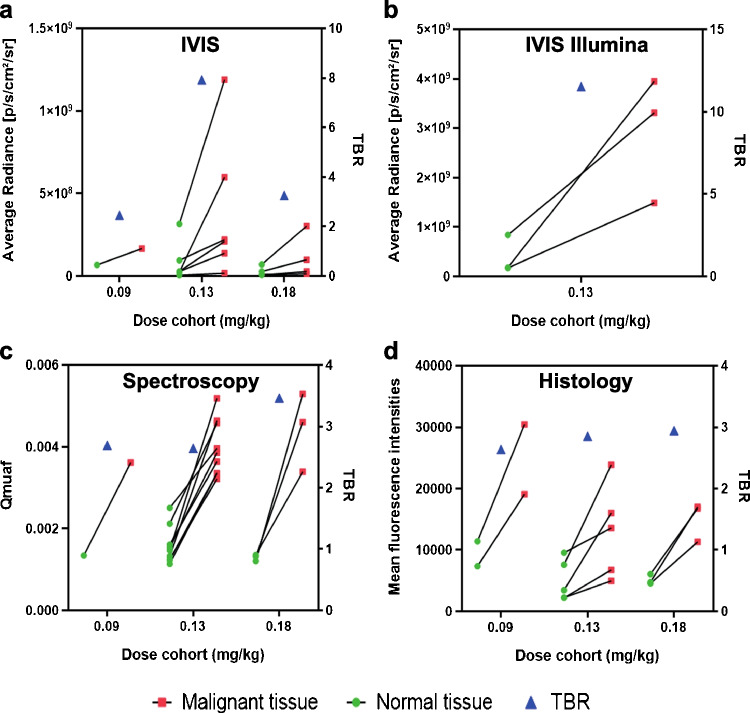
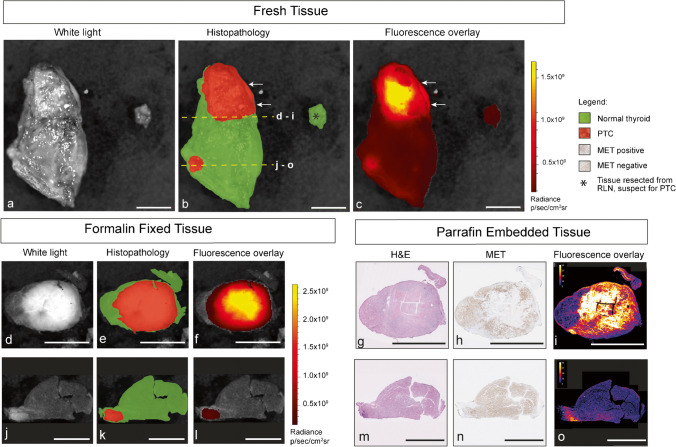
Results: Fourteen patients underwent hemi- or total thyroidectomy (TTX) after administration of 0.09 mg/kg (n = 1), 0.13 mg/kg (n = 8), or 0.18 mg/kg (n = 5) EMI-137. Both MFGI and spectroscopy could differentiate PTC from healthy thyroid tissue after administration of EMI-137, which binds selectively to MET in PTC. 0.13 mg/kg was the lowest dosage EMI-137 that allowed for differentiation between PTC and healthy thyroid tissue. The smallest PTC focus detected by MFGI was 1.4 mm. MFGI restaged 80% of patients from unifocal to multifocal PTC compared to ultrasound.
Conclusion: EMI-137-guided MFGI and spectroscopy can be used to detect multifocal PTC. This may improve disease staging and treatment selection between hemi- and total thyroidectomy by better differentiation between unifocal and multifocal disease.
Trial registration: NCT03470259.
Keywords: Molecular fluorescence–guided imaging; Multifocality; Papillary thyroid cancer; Spectroscopy.
© 2023. The Author(s).
Conflict of interest statement
GMvD is founder, shareholder, and CEO of TRACER Europe BV (Groningen, the Netherlands). None of the other authors reported any potential conflicts of interest.
Figures

References
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133. doi: 10.1089/thy.2015.0020. - DOI - PMC - PubMed
-
- Bongers PJ, Greenberg CA, Hsiao R, Vermeer M, Vriens MR, Lutke Holzik MF, et al. Differences in long-term quality of life between hemithyroidectomy and total thyroidectomy in patients treated for low-risk differentiated thyroid carcinoma. Surgery. 2020;167:94–101. doi: 10.1016/j.surg.2019.04.060. - DOI - PubMed
-
- Nickel B, Tan T, Cvejic E, Baade P, McLeod DSA, Pandeya N, et al. Health-related quality of life after diagnosis and treatment of differentiated thyroid cancer and association with type of surgical treatment. JAMA Otolaryngol Head Neck Surg. 2019;145:231. doi: 10.1001/jamaoto.2018.3870. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
