

Comparison of clinical outcomes in critically ill COVID-19 patients on mechanical ventilation with nosocomial pneumonia between Alpha and Omicron variants
- PMID: 38018405
- PMCID: PMC10685785
- DOI: 10.1177/17534666231213642
Comparison of clinical outcomes in critically ill COVID-19 patients on mechanical ventilation with nosocomial pneumonia between Alpha and Omicron variants
Abstract
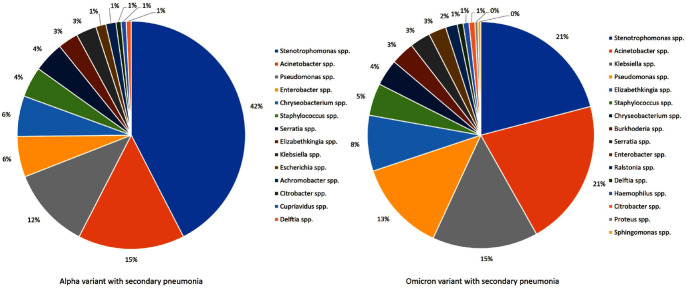
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes coronavirus disease 2019 (COVID-19), a pandemic that has resulted in millions of deaths worldwide. Critically ill COVID-19 patients who require intubation and develop nosocomial pneumonia, commonly caused by gram-negative bacilli, have a higher mortality rate than those without nosocomial pneumonia.
Objectives: The aim of this study is to compare the clinical characteristics and outcomes and associated risk factors of Alpha and Omicron SARS-CoV-2 variants in critically ill patients on mechanical ventilation (MV) with nosocomial pneumonia.
Design: This is a retrospective single-center cohort study.
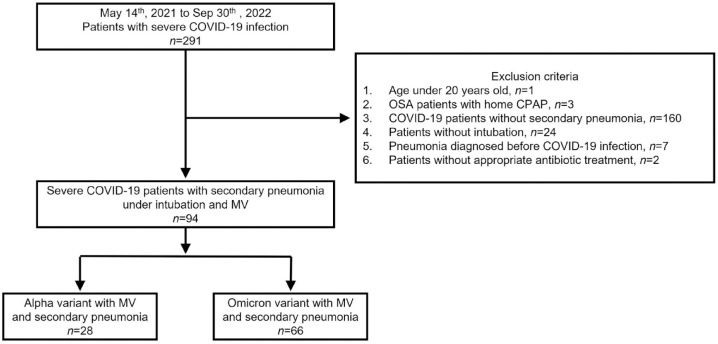
Methods: This observational study was conducted at Taipei Veterans General Hospital, Taiwan from May 2021 to September 2022. Critically ill patients who had confirmed SARS-CoV-2 infection and intubated on a MV with bacterial pneumonia were enrolled. Demographic data, laboratory results, and treatment information were collected and analyzed. In addition, clinical outcomes among different SARS-CoV-2 variants were examined.
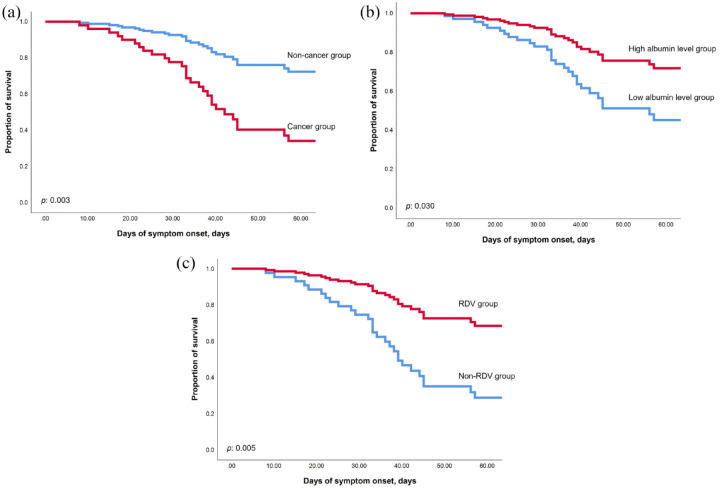
Results: This study included 94 critically ill COVID-19 patients who required intubation and intensive care unit (ICU) admission. The Alpha group had a longer duration of SARS-CoV-2 viral shedding, MV days, and ICU stay, while the Omicron group had older age, more comorbidities, higher APACHE II scores, and higher in-hospital mortality (47.0% versus 25.0%, p = 0.047). However, independent risk factors for in-hospital mortality included malignancy, lower serum albumin levels, and lack of Remdesivir treatment, except for the SARS-CoV-2 variant.
Conclusion: Our study discovered a higher in-hospital mortality rate in severe COVID-19 patients with MV and secondary pneumonia infected with the Omicron variant compared to the Alpha variant; however, real independent risk factors for in-hospital mortality are malignancy, lower serum albumin level, and lack of Remdesivir treatment.
Keywords: coronavirus disease 2019; hospital-acquired pneumonia; severe acute respiratory syndrome coronavirus 2 variants; ventilator-associated pneumonia.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
Similar articles
-
Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study.Lancet Respir Med. 2020 May;8(5):475-481. doi: 10.1016/S2213-2600(20)30079-5. Epub 2020 Feb 24. Lancet Respir Med. 2020. PMID: 32105632 Free PMC article.
-
Obesity May Not Be Associated with 28-Day Mortality, Duration of Invasive Mechanical Ventilation and Length of Intensive Care Unit and Hospital Stay in Critically Ill Patients with Severe Acute Respiratory Syndrome Coronavirus-2: A Retrospective Cohort Study.Medicina (Kaunas). 2021 Jun 29;57(7):674. doi: 10.3390/medicina57070674. Medicina (Kaunas). 2021. PMID: 34210077 Free PMC article.
-
Evaluation of characteristics and prognosis of COVID-19 patients requiring invasive mechanical ventilation during dominance of nonvariant, alpha, delta, and omicron variants in tertiary hospitals of Japan.BMC Infect Dis. 2024 Feb 20;24(1):223. doi: 10.1186/s12879-024-09131-4. BMC Infect Dis. 2024. PMID: 38374034 Free PMC article.
-
An observational study on factors associated with ICU mortality in Covid-19 patients and critical review of the literature.Sci Rep. 2023 May 13;13(1):7804. doi: 10.1038/s41598-023-34613-x. Sci Rep. 2023. PMID: 37179397 Free PMC article. Review.
-
Convalescent plasma or hyperimmune immunoglobulin for people with COVID-19: a rapid review.Cochrane Database Syst Rev. 2020 May 14;5(5):CD013600. doi: 10.1002/14651858.CD013600. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Jul 10;7:CD013600. doi: 10.1002/14651858.CD013600.pub2. PMID: 32406927 Free PMC article. Updated.
Cited by
-
Comparison of Clinical Characteristics and Mortality Outcome in Critical COVID-19 Patients Infected with Alpha and Omicron Variants.Infect Drug Resist. 2025 Jan 8;18:151-160. doi: 10.2147/IDR.S479896. eCollection 2025. Infect Drug Resist. 2025. PMID: 39803308 Free PMC article.
-
Influence of vaccination on critical COVID-19 patients with acute respiratory failure: a retrospective cohort study.Eur J Med Res. 2024 Apr 20;29(1):243. doi: 10.1186/s40001-024-01840-5. Eur J Med Res. 2024. PMID: 38643153 Free PMC article.
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
