

Effect of Noninvasive Airway Management of Comatose Patients With Acute Poisoning: A Randomized Clinical Trial
- PMID: 38019968
- PMCID: PMC10687712
- DOI: 10.1001/jama.2023.24391
Effect of Noninvasive Airway Management of Comatose Patients With Acute Poisoning: A Randomized Clinical Trial
Abstract
Importance: Tracheal intubation is recommended for coma patients and those with severe brain injury, but its use in patients with decreased levels of consciousness from acute poisoning is uncertain.
Objective: To determine the effect of intubation withholding vs routine practice on clinical outcomes of comatose patients with acute poisoning and a Glasgow Coma Scale score less than 9.
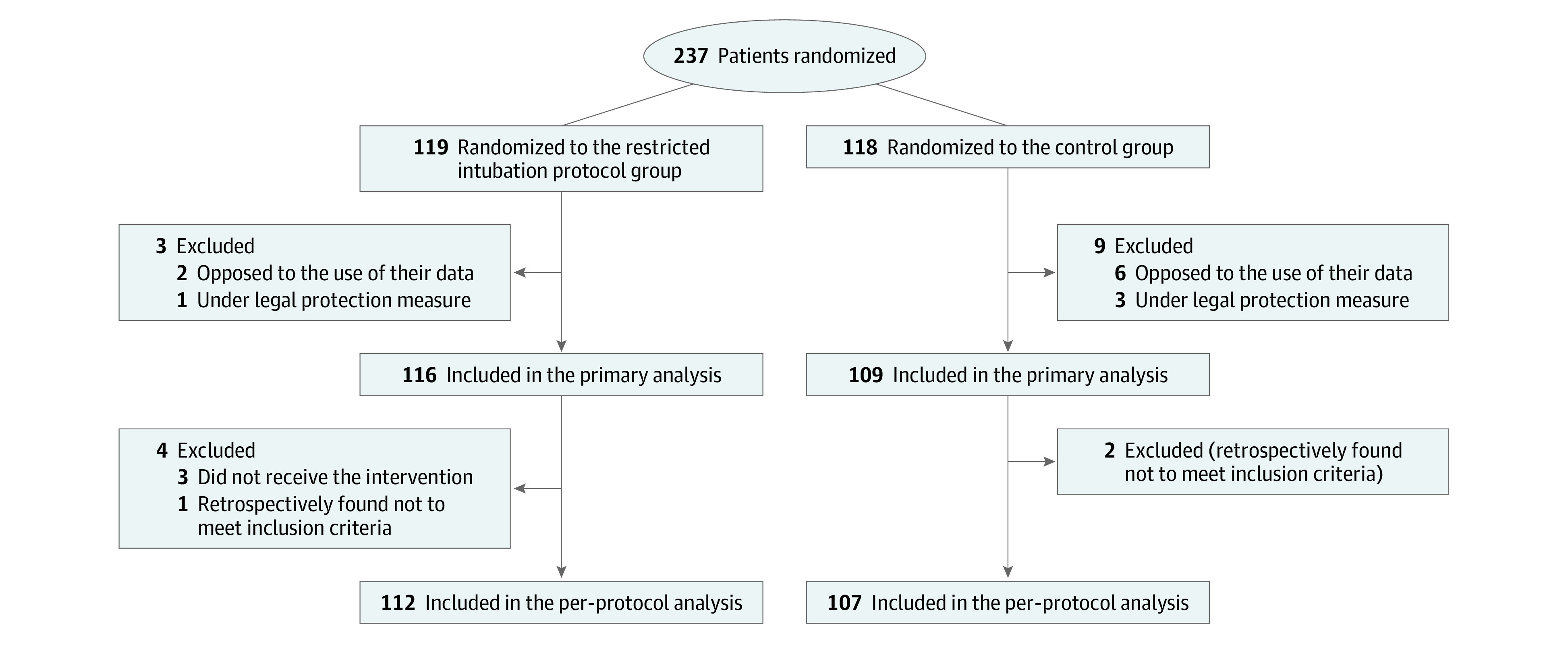
Design, setting, and participants: This was a multicenter, randomized trial conducted in 20 emergency departments and 1 intensive care unit (ICU) that included comatose patients with suspected acute poisoning and a Glasgow Coma Scale score less than 9 in France between May 16, 2021, and April 12, 2023, and followed up until May 12, 2023.
Intervention: Patients were randomized to undergo conservative airway strategy of intubation withholding vs routine practice.
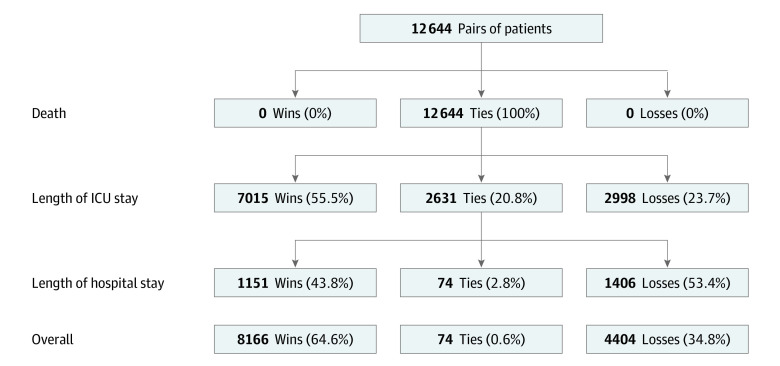
Main outcomes and measures: The primary outcome was a hierarchical composite end point of in-hospital death, length of ICU stay, and length of hospital stay. Key secondary outcomes included adverse events resulting from intubation as well as pneumonia within 48 hours.
Results: Among the 225 included patients (mean age, 33 years; 38% female), 116 were in the intervention group and 109 in the control group, with respective proportions of intubations of 16% and 58%. No patients died during the in-hospital stay. There was a significant clinical benefit for the primary end point in the intervention group, with a win ratio of 1.85 (95% CI, 1.33 to 2.58). In the intervention group, there was a lower proportion with any adverse event (6% vs 14.7%; absolute risk difference, 8.6% [95% CI, -16.6% to -0.7%]) compared with the control group, and pneumonia occurred in 8 (6.9%) and 16 (14.7%) patients, respectively (absolute risk difference, -7.8% [95% CI, -15.9% to 0.3%]).
Conclusions and relevance: Among comatose patients with suspected acute poisoning, a conservative strategy of withholding intubation was associated with a greater clinical benefit for the composite end point of in-hospital death, length of ICU stay, and length of hospital stay.
Trial registration: ClinicalTrials.gov Identifier: NCT04653597.
Conflict of interest statement
Figures
Comment in
-
The Value of Not Intubating Comatose Patients With Acute Poisoning.JAMA. 2023 Dec 19;330(23):2253-2254. doi: 10.1001/jama.2023.22462. JAMA. 2023. PMID: 38019975 No abstract available.
-
Does non-invasive airway management lead to better outcomes in comatose patients with suspected acute poisoning?CJEM. 2024 Apr;26(4):232-234. doi: 10.1007/s43678-024-00666-8. Epub 2024 Feb 13. CJEM. 2024. PMID: 38349503 No abstract available.
-
In patients with coma due to acute poisoning, withholding intubation improved clinical outcomes.Ann Intern Med. 2024 Apr;177(4):JC38. doi: 10.7326/J24-0011. Epub 2024 Apr 2. Ann Intern Med. 2024. PMID: 38560902
-
Noninvasive Airway Management of Comatose Patients With Acute Poisoning.JAMA. 2024 May 7;331(17):1504. doi: 10.1001/jama.2024.1423. JAMA. 2024. PMID: 38573611 No abstract available.
-
Noninvasive Airway Management of Comatose Patients With Acute Poisoning.JAMA. 2024 May 7;331(17):1504. doi: 10.1001/jama.2024.1426. JAMA. 2024. PMID: 38573629 No abstract available.
-
Noninvasive Airway Management of Comatose Patients With Acute Poisoning.JAMA. 2024 May 7;331(17):1502-1503. doi: 10.1001/jama.2024.1417. JAMA. 2024. PMID: 38573647 No abstract available.
-
Noninvasive Airway Management of Comatose Patients With Acute Poisoning.JAMA. 2024 May 7;331(17):1503-1504. doi: 10.1001/jama.2024.1429. JAMA. 2024. PMID: 38573650 No abstract available.
References
-
- Beaune S, Juvin P, Beauchet A, Casalino E, Megarbane B. Deliberate drug poisonings admitted to an emergency department in Paris area: a descriptive study and assessment of risk factors for intensive care admission. Eur Rev Med Pharmacol Sci. 2016;20(6):1174-1179. - PubMed
-
- Emergency management of poisoning. In: Shannon MW, Borron SW, Burns MJ, eds. Haddad and Winchester’s Clinical Management of Poisoning and Drug Overdose. 4th ed. WB Saunders. 2007:13-61. doi: 10.1016/B978-0-7216-0693-4.50007-4 - DOI
-
- Geeraerts T, Velly L, Abdennour L, et al. Prise en charge des traumatisés crâniens graves à la phase précoce (24 premières heures). In French. Anesthésie & Réanimation. 2016;2(6):431-453. doi: 10.1016/j.anrea.2016.09.007 - DOI
-
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative . The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453-1457. doi: 10.1016/S0140-6736(07)61602-X - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
