

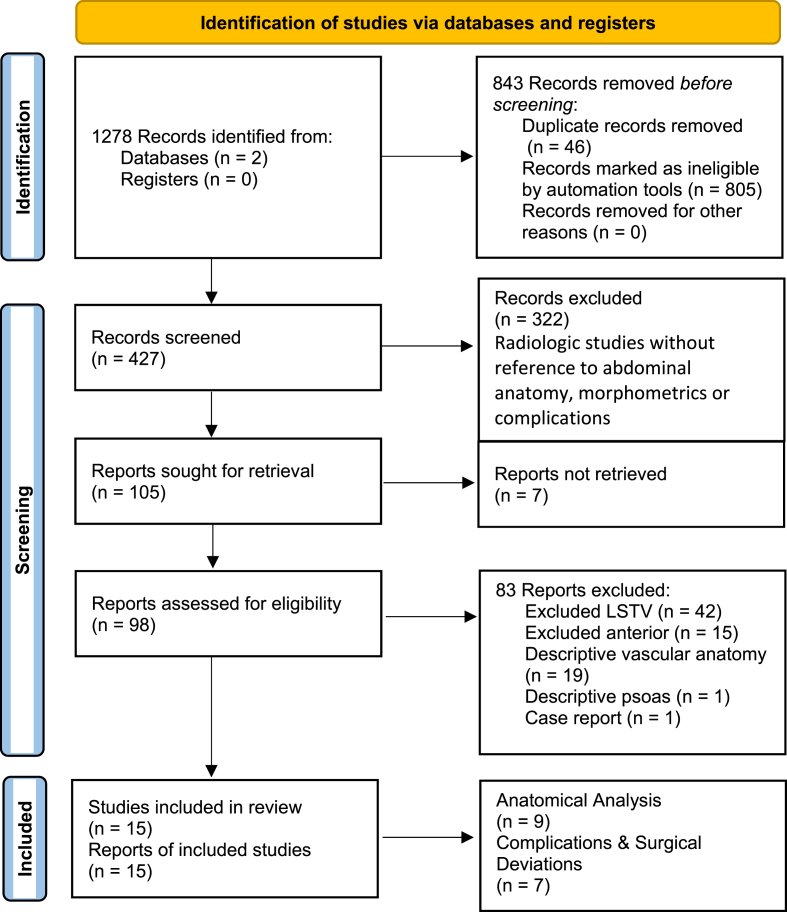
Anterior spinal fusion (ALIF/OLIF/LLIF) with lumbosacral transitional vertebra: A systematic review and proposed treatment algorithm
- PMID: 38021000
- PMCID: PMC10668067
- DOI: 10.1016/j.bas.2023.101713
Anterior spinal fusion (ALIF/OLIF/LLIF) with lumbosacral transitional vertebra: A systematic review and proposed treatment algorithm
Abstract
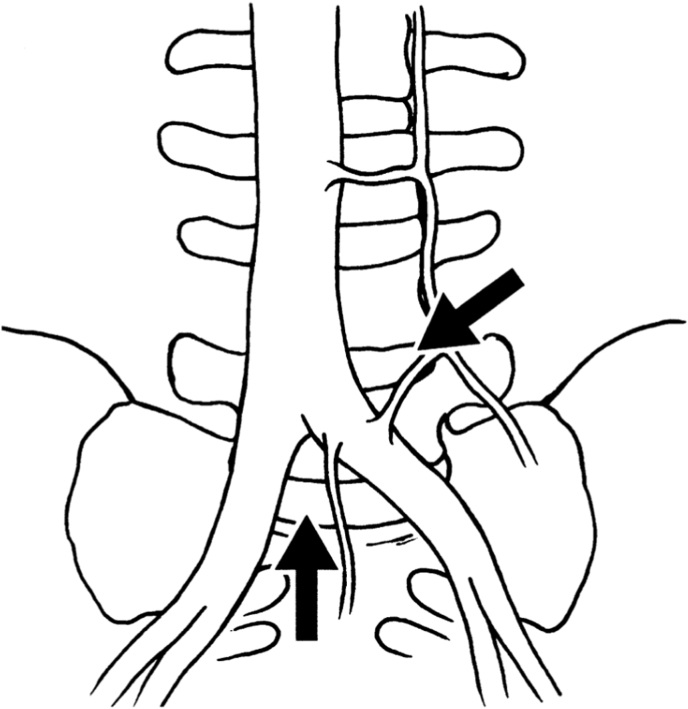
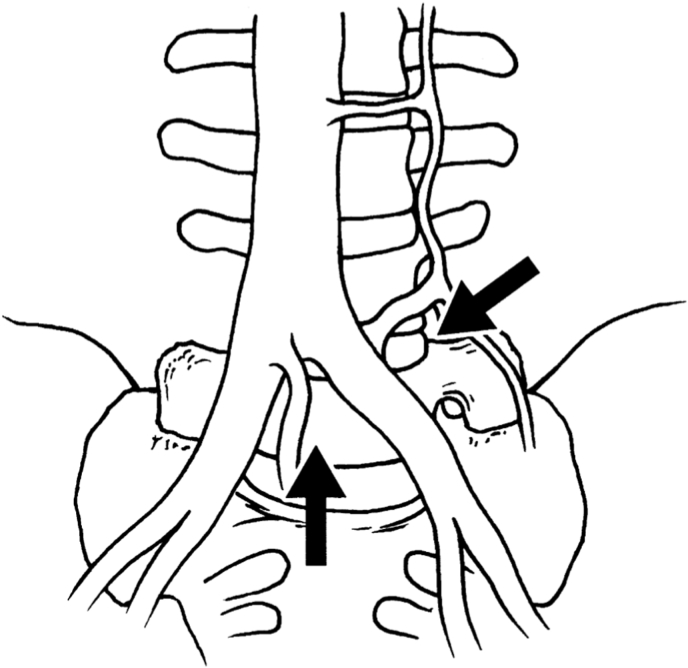
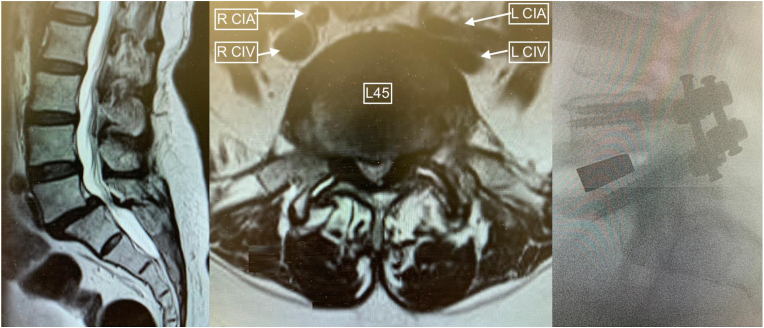
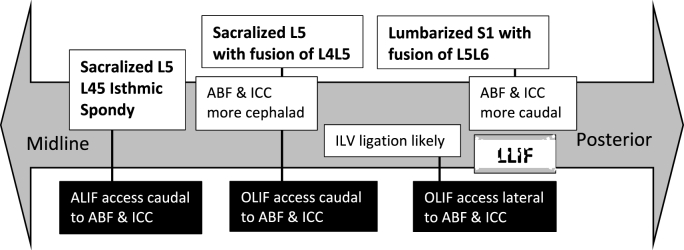
•Key anterior approaches differences in LSTV include vascular (aortic bifurcation/iliocaval confluence), muscular (psoas) and osseus anatomy (inter-crestal tangent/pubic symphysis), when compared to non-LSTV.•There are increased surgical deviations but not significantly greater complications for anterior approaches in LSTV.•Vascular awareness while accessing L45 will be in the presence of a more cephalad ABF and ICC with sacralized L5, and access to the deeper L56 level will be in the presence of a more caudal ABF and ICC in lumbarized S1.
Keywords: ABF; ALIF; ATP; Bertolotti; Castelvi; LLIF; Lumbarized; Lumbosacral transitional vertebrae; OLIF; Retroperitoneal; Sacralized.
© 2023 Published by Elsevier B.V. on behalf of EUROSPINE, the Spine Society of Europe, EANS, the European Association of Neurosurgical Societies.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

Similar articles
-
Approach-related anatomical differences in patients with lumbo-sacral transitional vertebrae undergoing lumbar fusion surgery at level L4/5.Arch Orthop Trauma Surg. 2023 Apr;143(4):1753-1759. doi: 10.1007/s00402-021-04303-2. Epub 2022 Jan 8. Arch Orthop Trauma Surg. 2023. PMID: 34999995 Free PMC article.
-
Risks Associated with Surgical Management of Lumbosacral Transitional Vertebrae: Systematic Review of Surgical Considerations and Illustrative Case.World Neurosurg. 2024 Jun;186:e54-e64. doi: 10.1016/j.wneu.2024.02.033. Epub 2024 Feb 11. World Neurosurg. 2024. PMID: 38350597
-
Technical description of oblique lateral interbody fusion at L1-L5 (OLIF25) and at L5-S1 (OLIF51) and evaluation of complication and fusion rates.Spine J. 2017 Apr;17(4):545-553. doi: 10.1016/j.spinee.2016.10.026. Epub 2016 Nov 21. Spine J. 2017. PMID: 27884744
-
Development of a novel in vitro cadaveric model for analysis of biomechanics and surgical treatment of Bertolotti syndrome.Spine J. 2020 Apr;20(4):638-656. doi: 10.1016/j.spinee.2019.10.011. Epub 2019 Oct 25. Spine J. 2020. PMID: 31669612
-
Oblique Lumbar Interbody Fusion: Technical Aspects, Operative Outcomes, and Complications.World Neurosurg. 2017 Feb;98:113-123. doi: 10.1016/j.wneu.2016.10.074. Epub 2016 Oct 21. World Neurosurg. 2017. PMID: 27777161 Review.
Cited by
-
The effects of cage on endplate collapse after stand-alone OLIF: based on finite element analysis and in vitro mechanics experiments.Front Bioeng Biotechnol. 2024 Dec 10;12:1508385. doi: 10.3389/fbioe.2024.1508385. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 39723127 Free PMC article.
-
Key Considerations in Surgical Decision-Making on the Side of Approach for Lumbar Lateral Transpsoas Interbody Fusion Techniques.Int J Spine Surg. 2025 May 12;19(2):145-155. doi: 10.14444/8721. Int J Spine Surg. 2025. PMID: 40049726 Free PMC article.
References
-
- Ahern D.P., Welch-Phillips A., Cawley D.T., Butler J.S. Is multilevel anterior lumbar interbody fusion (ALIF) superior to pedicle subtraction osteotomy (PSO) for degenerative lumbar deformity? Clinical Spine Surgery. 2020;33(1):1–4. Feb 1. - PubMed
-
- Aihara T., et al. Intervertebral disc degeneration associated with lumbosacral transitional vertebrae: a clinical and anatomical study. J. Bone Jt Surg. Br. 2005;87(5):687–691. - PubMed
-
- Bateman D.K., Millhouse P.W., Shahi N., Kadam A.B., Maltenfort M.G., Koerner J.D., Vaccaro A.R. Anterior lumbar spine surgery: a systematic review and meta-analysis of associated complications. Spine J. 2015;15(5):1118–1132. doi: 10.1016/j.spinee.2015.02.040. May 1. Epub 2015 Feb 26. PMID: 25728552. - DOI - PubMed
-
- Bron J.L., van Royen B.J., Wuisman P.I. The clinical significance of lumbosacral transitional anomalies. Acta Orthop. Belg. 2007;73:687–695. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
