

Small spheno-ethmoidal meningoencephalocele versus ethmoidal mucocele in spontaneous intracranial hypotension
- PMID: 38021026
- PMCID: PMC10668106
- DOI: 10.1016/j.bas.2023.102676
Small spheno-ethmoidal meningoencephalocele versus ethmoidal mucocele in spontaneous intracranial hypotension
Abstract
Background: Meningoencephalocele is defined as an abnormal sac of brain tissue and meninges extending beyond natural skull margins, often leading to cerebrospinal fluid (CSF) leakage. When this condition arises in the spheno-ethmoidal region, the diagnosis becomes more challenging as it can be mistaken for other nasal pathologies, such as mucocele.
Research question: We show in this case report a non-congenital sphenoethmoidal meningoencephalocele causing rhinoliquoral fistula and spontaneous intracranial hypotension.
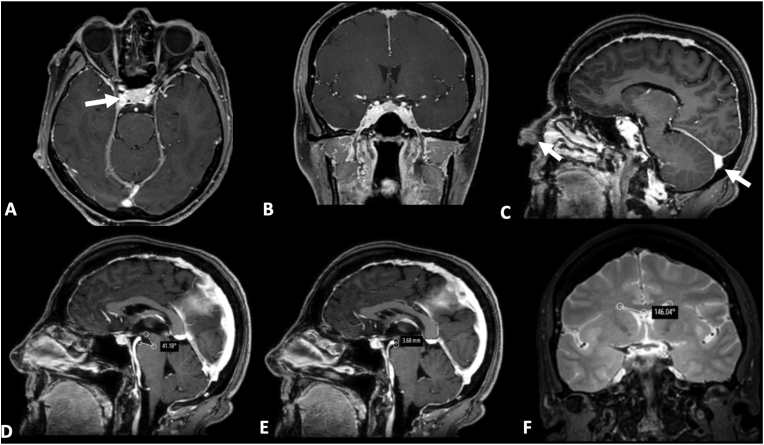
Results: this 65-year-old woman presented with sporadic rhinoliquorrhoea associated with orthostatic headache, nausea and dizziness. Brain MRI revealed a small lesion of an ethmoidal sinus, which was successfully treated with endoscopic endonasal surgery. Histology confirmed the presence of meningoencephalic tissue positive for S100 protein on immunohistochemistry.
Conclusions: When dealing with lesions of the paranasal sinuses in contact with the anterior skull base, rhinoliquorrhoea presence suggests meningoencephalocele. In dubious cases, a proper workup, including a thorough clinical history and neurological examination, specific imaging, and a direct search of CSF-like markers, is essential to support the differential diagnosis. In such cases, a transnasal endoscopic surgical approach is recommended to obtain a final histological diagnosis and to perform eventual dural plastic surgery.
Keywords: Cerebrospinal fluid leak; Meningoencephalocele; Mucocele; Orthostatic headache; Rhinoliquorrhoea; Spontaneous intracranial hypotension.
© 2023 The Authors.
Figures

References
-
- Abdel-Aziz M., El-Bosraty H., Qotb M., El-Hamamsy M., El-Sonbaty M., Abdel-Badie H., et al. Nasal encephalocele: endoscopic excision with anesthetic consideration. Int. J. Pediatr. Otorhinolaryngol. 2010;74(8):869–873. - PubMed
-
- Beckhardt R.N., Setzen M., Carras R. Primary spontaneous cerebrospinal fluid rhinorrhea. Otolaryngol. Head Neck Surg. 1991;104(4):425–432. - PubMed
-
- Blaivie C., Lequeux T., Kampouridis S., Louryan S., Saussez S. Congenital transsphenoidal meningocele: case report and review of the literature. Am. J. Otolaryngol. 2006;27(6):422–424. - PubMed
-
- Brook I., Frazier E.H. The microbiology of mucopyocele. Laryngoscope. 2001;111(10) https://pubmed.ncbi.nlm.nih.gov/11801943/ [Internet] 1771–3. Available from: - PubMed
-
- Brunori A., Bruni P., Delitala A., Greco R., Chiappetta F. Frontoethmoidal osteoma complicated by intracranial mucocele and hypertensive pneumocephalus: case report. Neurosurgery. 1995;36:1237–1238. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
