

Integrated analysis of randomized controlled trials evaluating bortezomib + lenalidomide + dexamethasone or bortezomib + thalidomide + dexamethasone induction in transplant-eligible newly diagnosed multiple myeloma
- PMID: 38023148
- PMCID: PMC10652744
- DOI: 10.3389/fonc.2023.1197340
Integrated analysis of randomized controlled trials evaluating bortezomib + lenalidomide + dexamethasone or bortezomib + thalidomide + dexamethasone induction in transplant-eligible newly diagnosed multiple myeloma
Abstract
Objective: Providing the most efficacious frontline treatment for newly diagnosed multiple myeloma (NDMM) is critical for patient outcomes. No direct comparisons have been made between bortezomib + lenalidomide + dexamethasone (VRD) and bortezomib + thalidomide + dexamethasone (VTD) induction regimens in transplant-eligible NDMM.
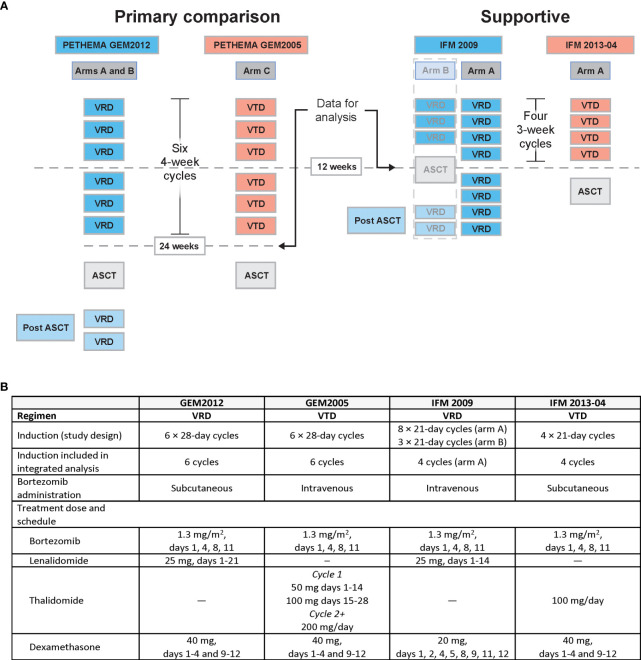
Methods: An integrated analysis was performed using patient data from four trials meeting prespecified eligibility criteria: two using VRD (PETHEMA GEM2012 and IFM 2009) and two using VTD (PETHEMA GEM2005 and IFM 2013-04).
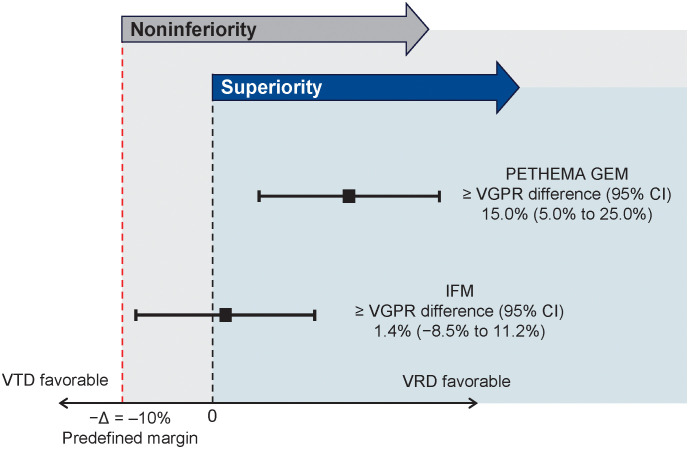
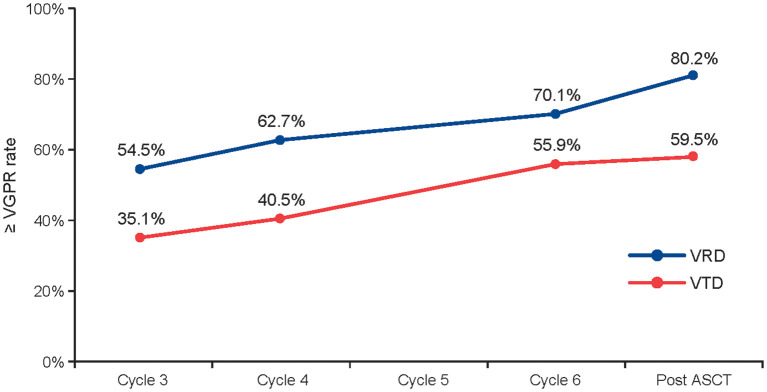
Results: The primary endpoint was met, with VRD demonstrating a noninferior rate of at least very good partial response (≥ VGPR) after induction vs VTD. GEM comparison demonstrated improvement in the ≥ VGPR rate after induction for VRD vs VTD (66.3% vs 51.2%; P = .00281) that increased after transplant (74.4% vs 53.5%). Undetectable minimal residual disease rates post induction (46.7% vs 34.9%) and post transplant (62.4% vs 47.3%) support the benefit of VRD vs VTD. Treatment-emergent adverse events leading to study and/or treatment discontinuation were less frequent with VRD (3%, GEM2012; 6%, IFM 2009) vs VTD (11%, IFM 2013-04).
Conclusion: These results supported the benefit of VRD over VTD for induction in transplant-eligible patients with NDMM. The trials included are registered with ClinicalTrials.gov (NCT01916252, NCT01191060, NCT00461747, and NCT01971658).
Keywords: bortezomib; dexamethasone; lenalidomide; multiple myeloma; thalidomide.
Copyright © 2023 Rosiñol, Hebraud, Oriol, Colin, Ríos Tamayo, Hulin, Blanchard, Caillot, Sureda, Hernández, Arnulf, Mateos, Macro, San-Miguel, Belhadj, Lahuerta, Garelik, Bladé and Moreau.
Conflict of interest statement
LR and JL report honoraria from Janssen; Celgene, a Bristol-Myers Squibb Company; Takeda; and Amgen. AO reports consultancy and speakers bureau with Amgen; Janssen; Takeda; and Celgene, a Bristol-Myers Squibb Company. RR reports consultancy with Amgen; Celgene, a Bristol-Myers Squibb Company; Janssen; and Takeda. CH reports honoraria from Celgene, a Bristol-Myers Squibb Company; Janssen; Takeda; and Amgen. AS reports honoraria from Bristol Myers Squibb, Takeda, Sanofi, Merck, and Roche; consultancy with Bristol Myers Squibb, Takeda, and Merck; and speakers bureau with Takeda. M-VM reports honoraria and membership on advisory boards with Janssen; Celgene, a Bristol-Myers Squibb Company; Amgen; Takeda; AbbVie; GlaxoSmithKline; EDO; PharmaMar; and Adaptive. MM reports honoraria, membership on advisory boards, and financial support with Celgene, a Bristol-Myers Squibb Company; Janssen; and Takeda and honoraria and membership on advisory boards with Amgen. JS-M reports consultancy with Bristol Myers Squibb; Celgene, a Bristol-Myers Squibb Company; Novartis; Takeda; Amgen; MSD; Janssen; and Sanofi and membership on board of directors or advisory committees with Takeda. KB reports honoraria and consultancy with Celgene, a Bristol-Myers Squibb Company; Amgen; Janssen; and Takeda. MG reports employment with Celgene, a Bristol-Myers Squibb Company. JB reports honoraria from Janssen; Celgene, a Bristol-Myers Squibb Company; and Amgen. PM reports honoraria from Celgene, a Bristol-Myers Squibb Company; Janssen; Takeda; AbbVie; and Amgen. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declare that this study received funding from Celgene, a Bristol-Myers Squibb Company. Author MG was employed by the funder and involved in study design, collection, analysis, or interpretation of data and writing the article and deciding to submit the article for publication.
Figures
References
-
- Surveillance Epidemiology and End Results (SEER): National Cancer Institute (2014). Available at: http://seer.cancer.gov.
-
- Dimopoulos MA, Moreau P, Terpos E, Mateos MV, Zweegman S, Cook G, et al. Multiple myeloma: EHA-ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Hemasphere (2021) 5(2):e528. Available at: http://journals.lww.com/hemasphere/fulltext/2021/02000/multiple_myeloma_.... - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous