

Longitudinal characteristics of T2-FLAIR mismatch in IDH-mutant astrocytomas: Relation to grade, histopathology, and overall survival in the GLASS-NL cohort
- PMID: 38024241
- PMCID: PMC10681663
- DOI: 10.1093/noajnl/vdad149
Longitudinal characteristics of T2-FLAIR mismatch in IDH-mutant astrocytomas: Relation to grade, histopathology, and overall survival in the GLASS-NL cohort
Abstract
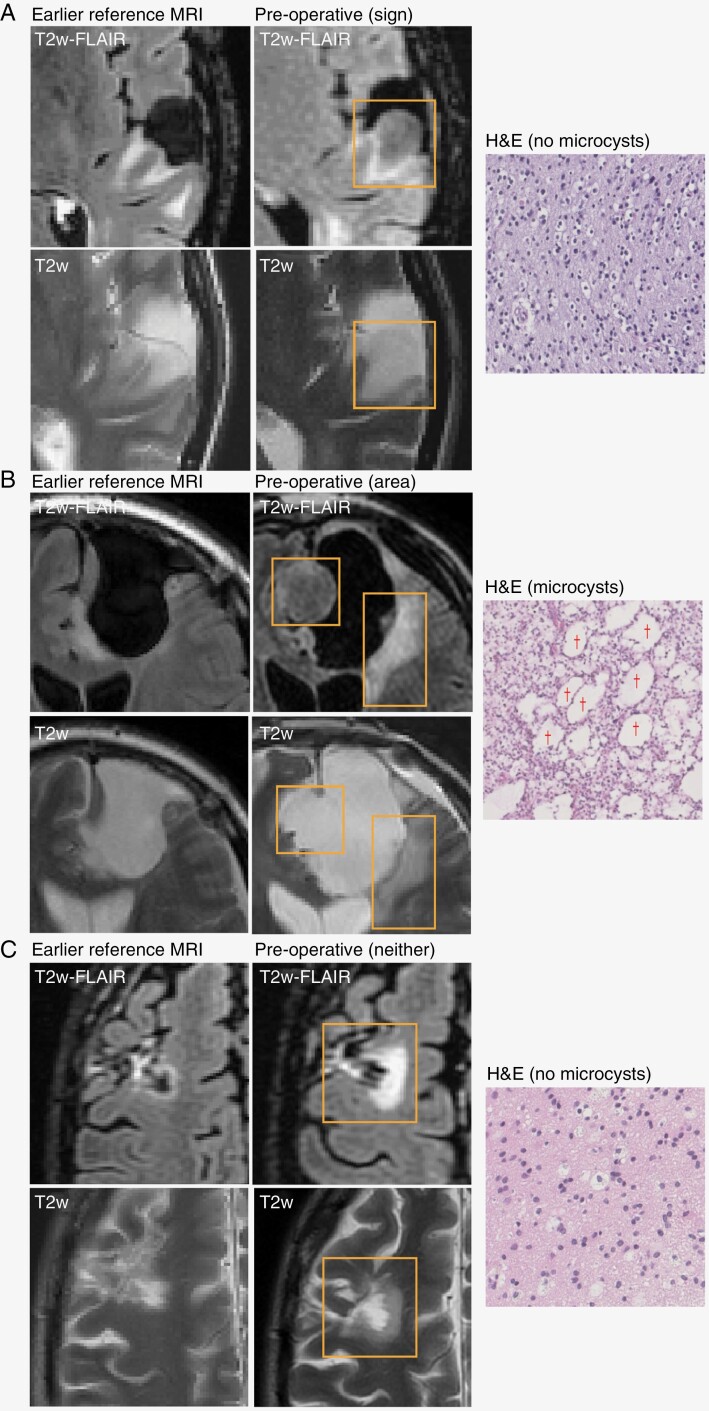
Background: The T2-FLAIR mismatch sign is defined by signal loss of the T2-weighted hyperintense area with Fluid-Attenuated Inversion Recovery (FLAIR) on magnetic resonance imaging, causing a hypointense region on FLAIR. It is a highly specific diagnostic marker for IDH-mutant astrocytoma and is postulated to be caused by intercellular microcystic change in the tumor tissue. However, not all IDH-mutant astrocytomas show this mismatch sign and some show the phenomenon in only part of the lesion. The aim of the study is to determine whether the T2-FLAIR mismatch phenomenon has any prognostic value beyond initial noninvasive molecular diagnosis.
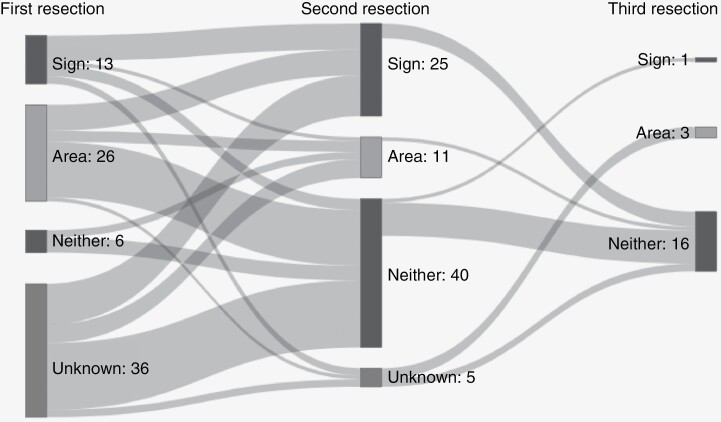
Methods: Patients initially diagnosed with histologically lower-grade (2 or 3) IDH-mutant astrocytoma and with at least 2 surgical resections were included in the GLASS-NL cohort. T2-FLAIR mismatch was determined, and the growth pattern of the recurrent tumor immediately before the second resection was annotated as invasive or expansive. The relation between the T2-FLAIR mismatch sign and tumor grade, microcystic change, overall survival (OS), and other clinical parameters was investigated both at first and second resection.
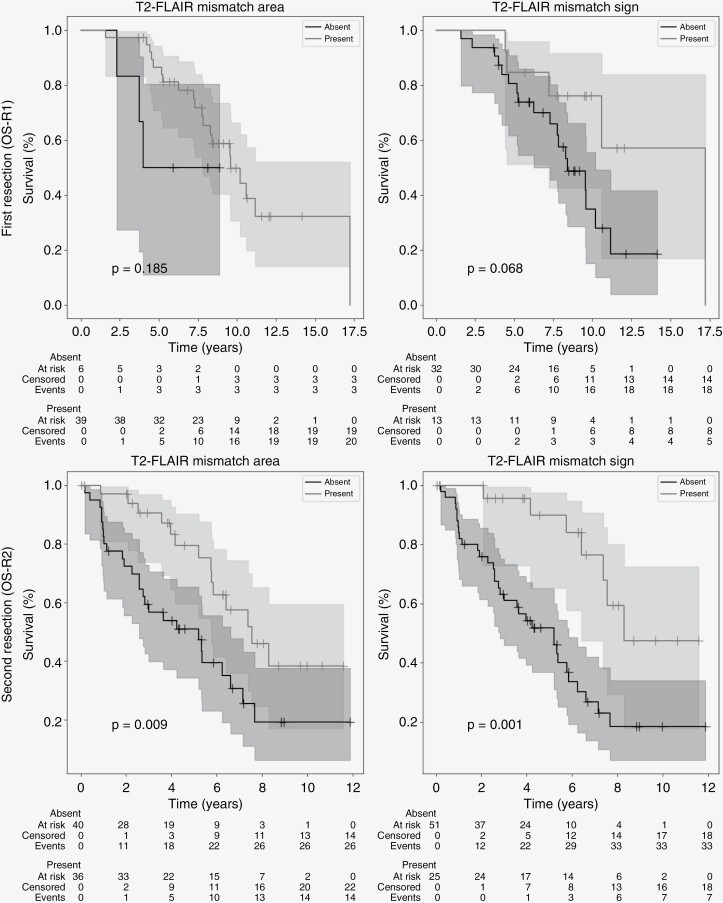
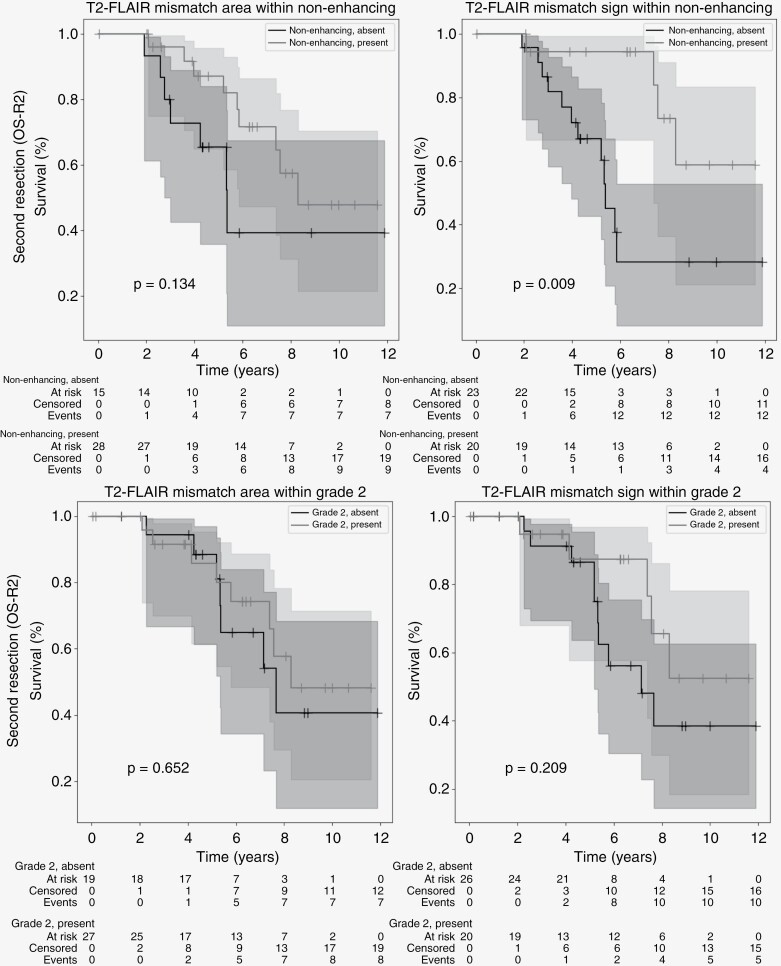
Results: The T2-FLAIR mismatch sign was significantly related to Grade 2 (80% vs 51%), longer post-resection median OS (8.3 vs 5.2 years), expansive growth, and lower age at second resection. At first resection, no relation was found between the mismatch sign and OS. Microcystic change was associated with areas of T2-FLAIR mismatch.
Conclusions: T2-FLAIR mismatch in IDH-mutant astrocytomas is correlated with microcystic change in the tumor tissue, favorable prognosis, and Grade 2 tumors at the time of second resection.
Keywords: astrocytoma; glioma; magnetic resonance imaging.
© The Author(s) 2023. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Conflict of interest statement
M.S. reports receiving speaker fees (paid to the institution) from GE Health care and AuntMinnie.com, and consulting fees (paid to the institution) from Bracco SpA. The other authors declare no conflicts of interest.
Figures
References
-
- Patel SH, Poisson LM, Brat DJ, et al. . T2–FLAIR mismatch, an imaging biomarker for IDH and 1p/19q status in lower-grade gliomas: a TCGA/TCIA project. Clin Cancer Res. 2017;23(20):6078–6085. - PubMed
LinkOut - more resources
Full Text Sources