

Assessing GFR With Proenkephalin
- PMID: 38025210
- PMCID: PMC10658254
- DOI: 10.1016/j.ekir.2023.08.006
Assessing GFR With Proenkephalin
Abstract
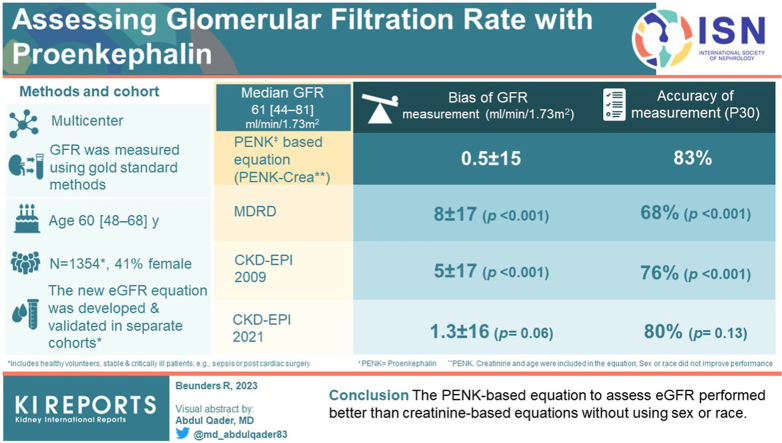
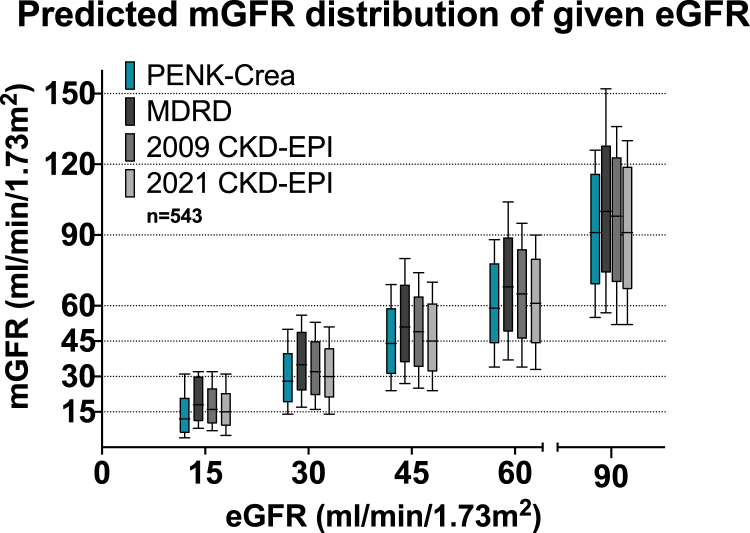
Introduction: In clinical practice, kidney (dys)function is monitored through creatinine-based estimations of glomerular filtration rate (eGFR: Modification of Diet in Renal Disease [MDRD], Chronic Kidney Disease Epidemiology Collaboration [CKD-EPI]). Creatinine is recognized as a late and insensitive biomarker of glomerular filtration rate (GFR). The novel biomarker proenkephalin (PENK) may overcome these limitations, but no PENK-based equation for eGFR is currently available. Therefore, we developed and validated a PENK-based equation to assess GFR.
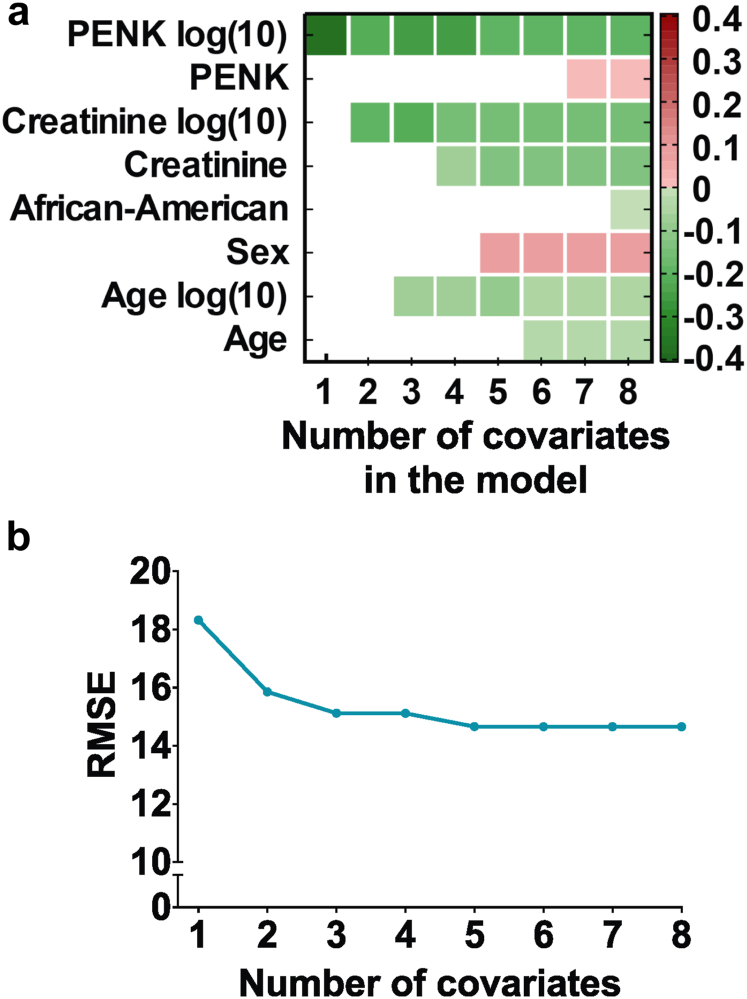
Methods: In this international multicenter study in 1354 stable and critically ill patients, GFR was measured (mGFR) through iohexol or iothalamate clearance. A generalized linear model with sigmoidal nonlinear transfer function was used for equation development in the block-randomized development set. Covariates were selected in a data-driven fashion. The novel equation was assessed for bias, precision (mean ± SD), and accuracy (eGFR percentage within ±30% of mGFR, P30) in the validation set and compared with MDRD and CKD-EPI.
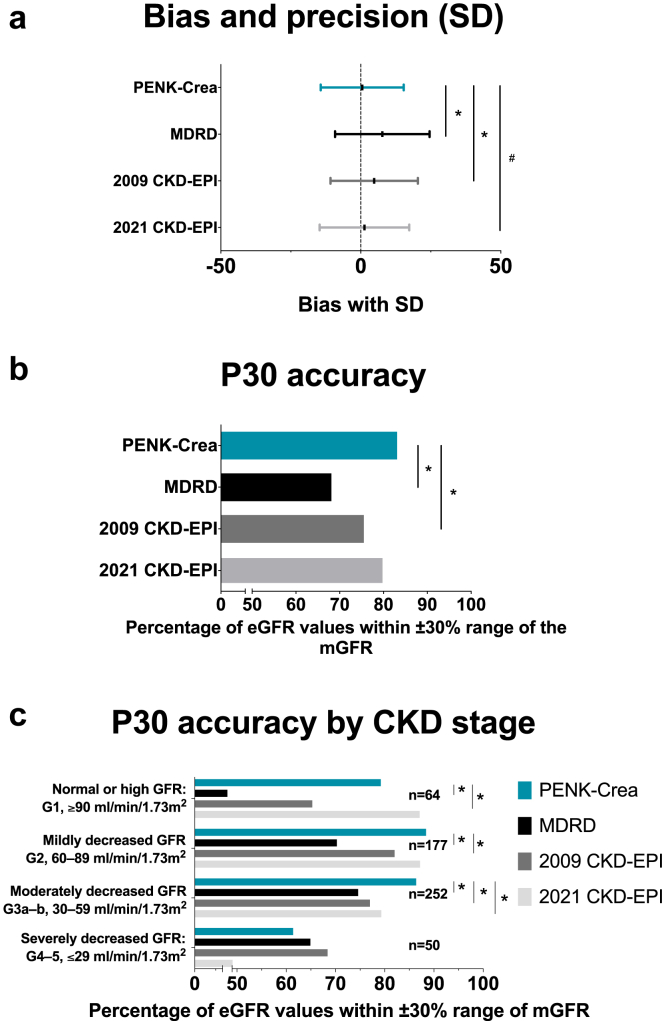
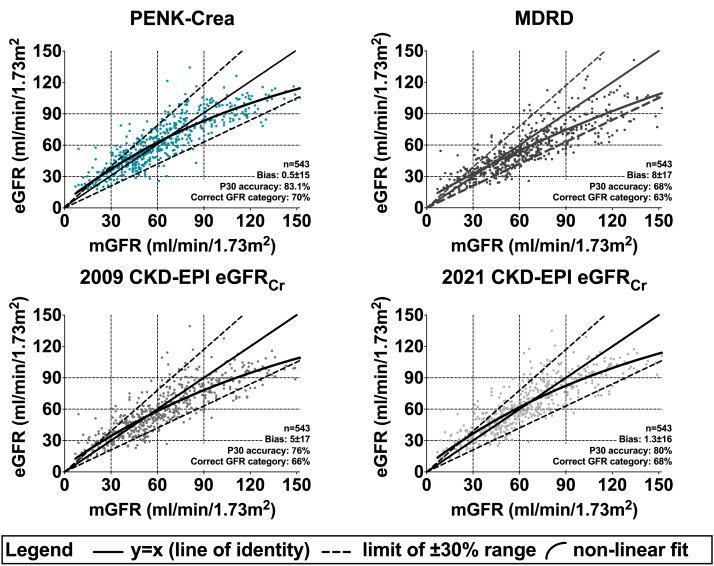
Results: Median mGFR was 61 [44-81] ml/min per 1.73 m2. In order of importance, PENK, creatinine, and age were included, and sex or race did not improve performance. The PENK-based equation mean ± SD bias of the mGFR was 0.5 ± 15 ml/min per 1.73 m2, significantly less compared with MDRD (8 ± 17, P < 0.001) and 2009 CKD-EPI (5 ± 17, P < 0.001), not reaching statistical significance compared with 2021 CKD-EPI (1.3 ± 16, P = 0.06). The P30 accuracy of the PENK-based equation was 83%, significantly higher compared with MDRD (68%, P < 0.001) and 2009 CKD-EPI (76%, P < 0.001), similar to 2021 CKD-EPI (80%, P = 0.13).
Conclusion: Overall, the PENK-based equation to assess eGFR performed better than most creatinine-based equations without using sex or race.
Keywords: acute kidney injury; creatinine; estimated glomerular filtration rate; gold standard; kidney function; proenkephalin.
© 2023 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
