

Prospective Cohort Study of Soluble Urokinase Plasminogen Activation Receptor and Cardiovascular Events in Patients With CKD
- PMID: 38025216
- PMCID: PMC10658273
- DOI: 10.1016/j.ekir.2023.08.038
Prospective Cohort Study of Soluble Urokinase Plasminogen Activation Receptor and Cardiovascular Events in Patients With CKD
Abstract
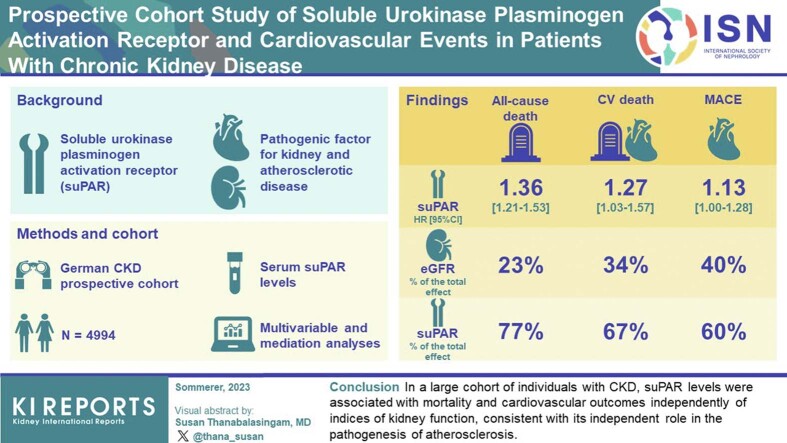
Introduction: Soluble urokinase plasminogen activation receptor (suPAR) is an immune-derived pathogenic factor for kidney and atherosclerotic disease. Whether the association between suPAR and cardiovascular (CV) outcomes is dependent on the severity of underlying kidney disease is unclear.
Methods: We measured serum suPAR levels in 4994 participants (mean age 60 years; 60% men; 36% with diabetes mellitus; mean estimated glomerular filtration rate (eGFR) 49 ml/min per 1.73 m2, SD 18) of the German Chronic Kidney Disease (GCKD) cohort and examined its association with all-cause death, CV death, and major CV events (MACE) across the range of eGFR and urine albumin-to-creatinine ratio (UACR).
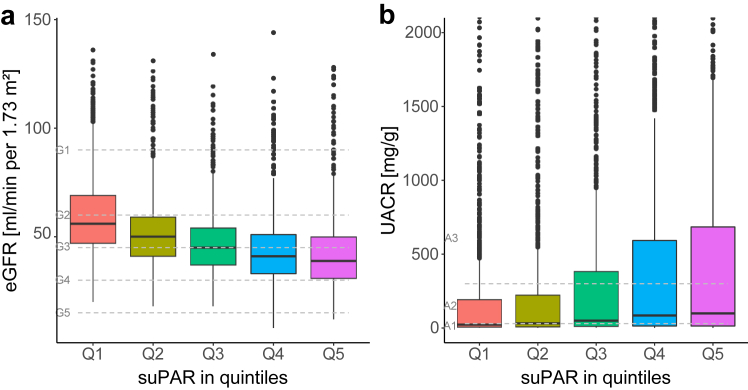
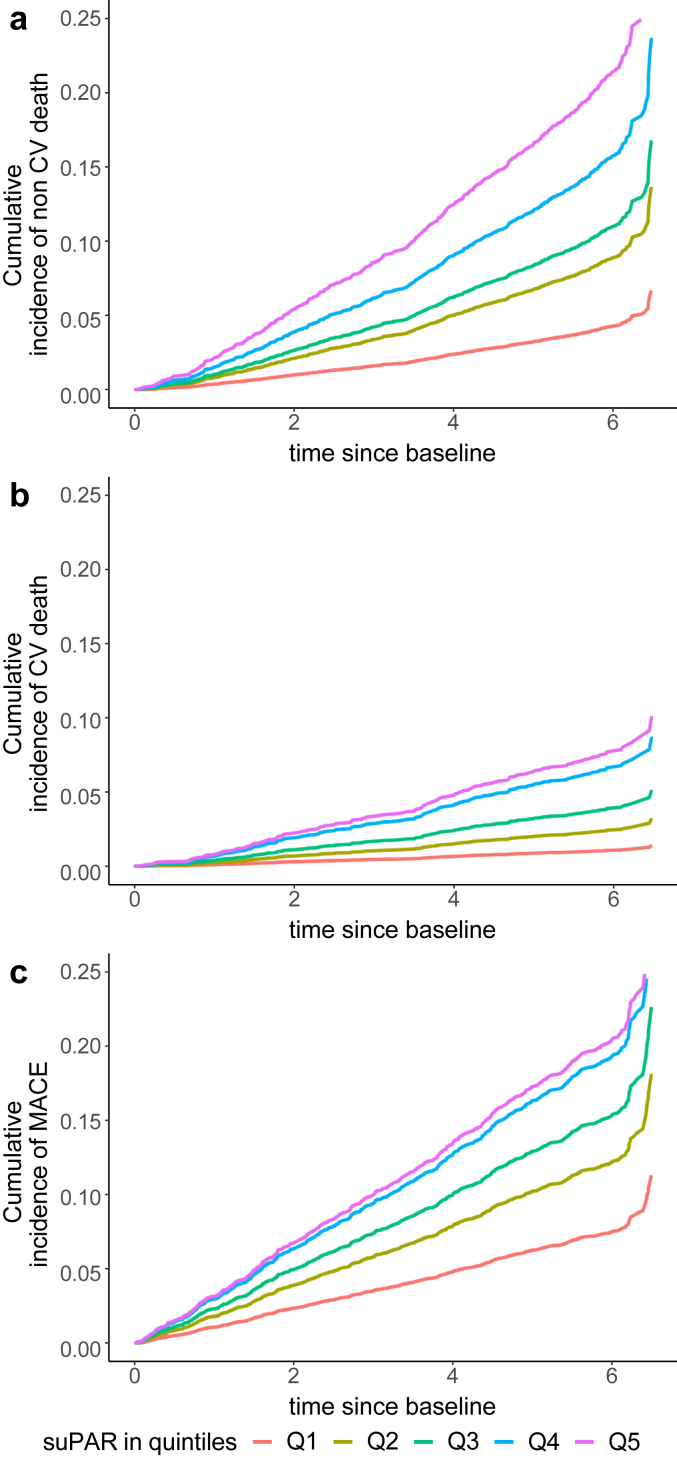
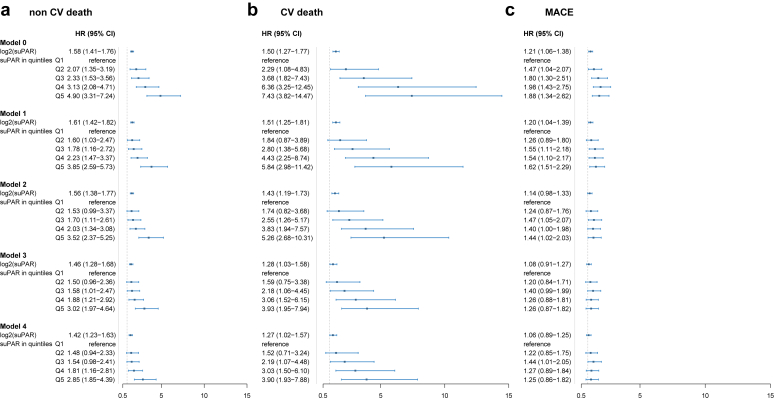
Results: The median suPAR level was 1771 pg/ml (interquartile range [IQR] 1447-2254 pg/ml). SuPAR levels were positively and independently correlated with age, eGFR, UACR, and parathyroid hormone levels. There were 573 deaths, including 190 CV deaths and 683 MACE events at a follow-up time of 6.5 years. In multivariable analyses, suPAR levels (log2) were associated with all-cause death (hazard ratio [HR] 1.36, 95% confidence interval [CI] 1.21-1.53), CV death (HR 1.27, 95% CI 1.03-1.57), and MACE (HR 1.13, 95% CI 1.00-1.28), and were not found to differ according to diabetes mellitus status, baseline eGFR, UACR, or parathyroid hormone levels. In mediation analysis, suPAR's direct effect on all-cause death, CV death, and MACE accounted for 77%, 67%, and 60% of the total effect, respectively; whereas the effect mediated through eGFR accounted for 23%, 34%, and 40%, respectively.
Conclusion: In a large cohort of individuals with chronic kidney disease (CKD), suPAR levels were associated with mortality and CV outcomes independently of indices of kidney function, consistent with its independent role in the pathogenesis of atherosclerosis.
Keywords: biomarkers; cardiovascular outcomes; cohort; eGFR; suPAR; uACR.
© 2023 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
