

Focal Segmental Glomerulosclerosis: Assessing the Risk of Relapse
- PMID: 38025232
- PMCID: PMC10658237
- DOI: 10.1016/j.ekir.2023.08.035
Focal Segmental Glomerulosclerosis: Assessing the Risk of Relapse
Abstract
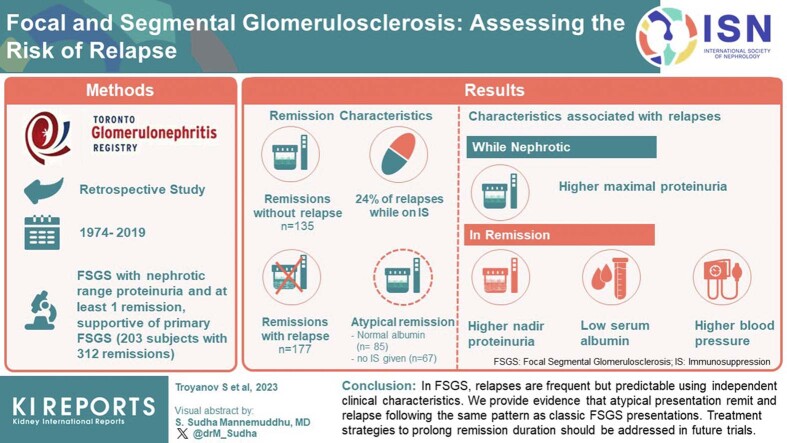
Introduction: Kidney outcomes are improved in primary focal segmental glomerulosclerosis (FSGS) by maintaining a remission in proteinuria. However, characteristics associated with relapses are uncertain. We sought to identify these by analyzing each remission.
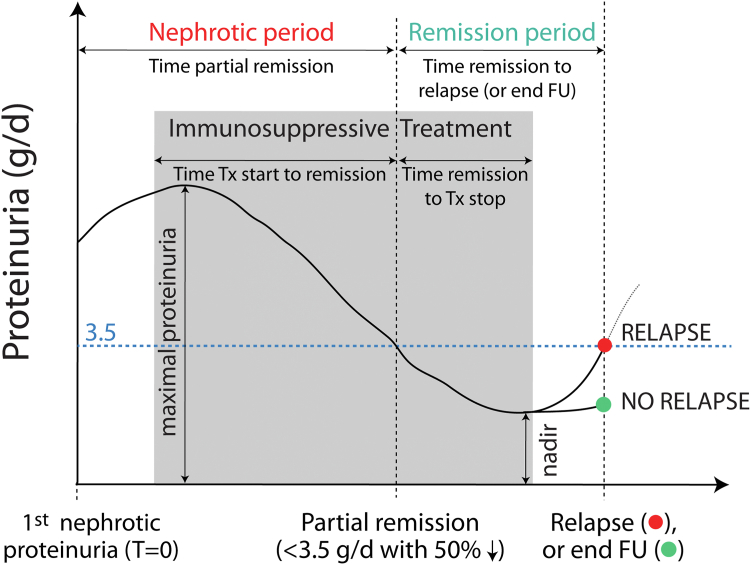
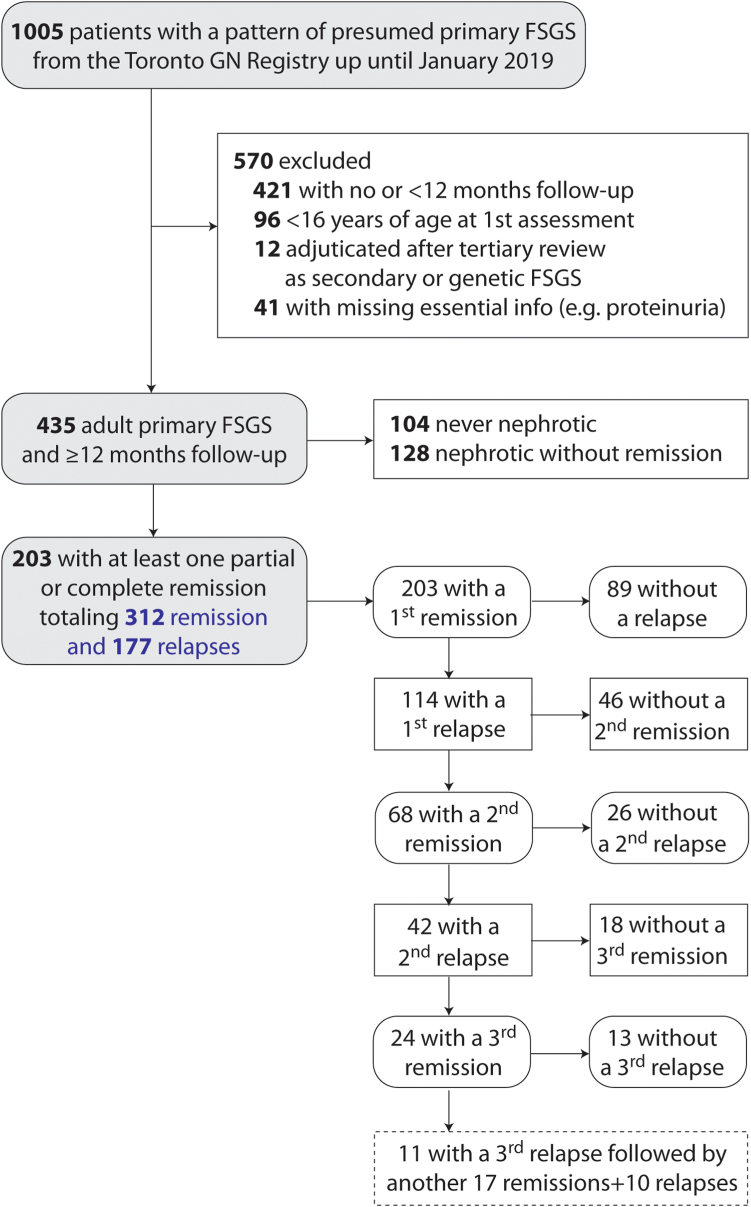
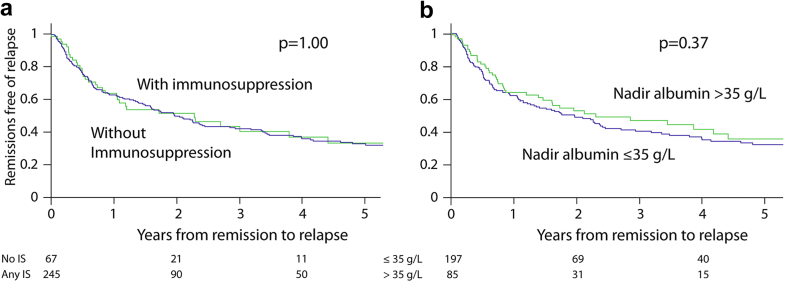
Methods: We performed a retrospective study in patients with biopsy-proven lesions of FSGS, absent identifiable secondary cause, who had at least 1 remission from nephrotic-range proteinuria. In each patient, we identified every remission, every relapse, and their durations. Using a multilevel logistic regression to account for the clustering of multiple remissions within a patient, we tested which clinical characteristics were independently associated with relapses.
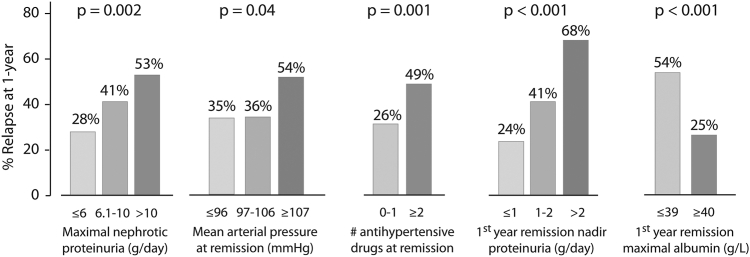
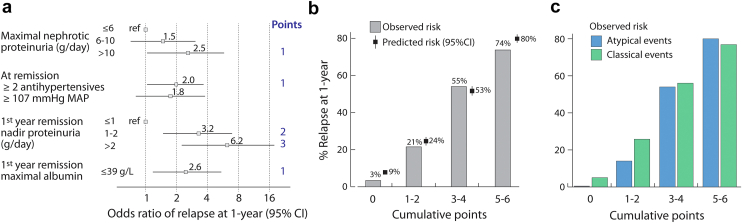
Results: In 203 individuals, 312 remissions occurred, 177 with and 135 without relapse. A minority of remissions were atypical, defined by either absent hypoalbuminemia and/or no immunosuppression (IS), in contrast to the classic nephrotic syndrome that remits with IS. Atypical remission variants were just as likely to relapse as the classical presentation. Only 24% of remission events were on maintenance therapy at relapse. Independent characteristics associated with relapses were higher maximal proteinuria while nephrotic; and in remission, higher nadir proteinuria, lower serum albumin, and higher blood pressure. Using these variables, we created a tool estimating the 1-year risk of relapse ranging from 9% to 80%, well-calibrated to the observed data.
Conclusion: In FSGS, relapses are frequent but predictable using independent clinical characteristics. We also provide evidence that atypical presentations remit and relapse following the same pattern as classic FSGS presentations. Treatment strategies to prolong remission duration should be addressed in future trials.
Keywords: FSGS; albuminemia; event-analysis; immunosuppression; proteinuria; relapse.
© 2023 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
LinkOut - more resources
Full Text Sources
