

The benefit of complete resection of contrast enhancing tumor in glioblastoma patients: A population-based study
- PMID: 38026582
- PMCID: PMC10666813
- DOI: 10.1093/nop/npad037
The benefit of complete resection of contrast enhancing tumor in glioblastoma patients: A population-based study
Abstract
Background: New treatment modalities have not been widely adopted for patients with glioblastoma (GBM) after the addition of temozolomide to radiotherapy. We hypothesize that increased extent of resection (EOR) has resulted in improved survival for surgically treated patients with glioblastoma at the population level.
Methods: Retrospective analysis of adult patients operated for glioblastoma in the population of South-Eastern Norway. Patients were stratified into Pre-temozolomide- (2003-2005), temozolomide- (2006-2012), and resection-focused period (2013-2019) and evaluated according to age and EOR.
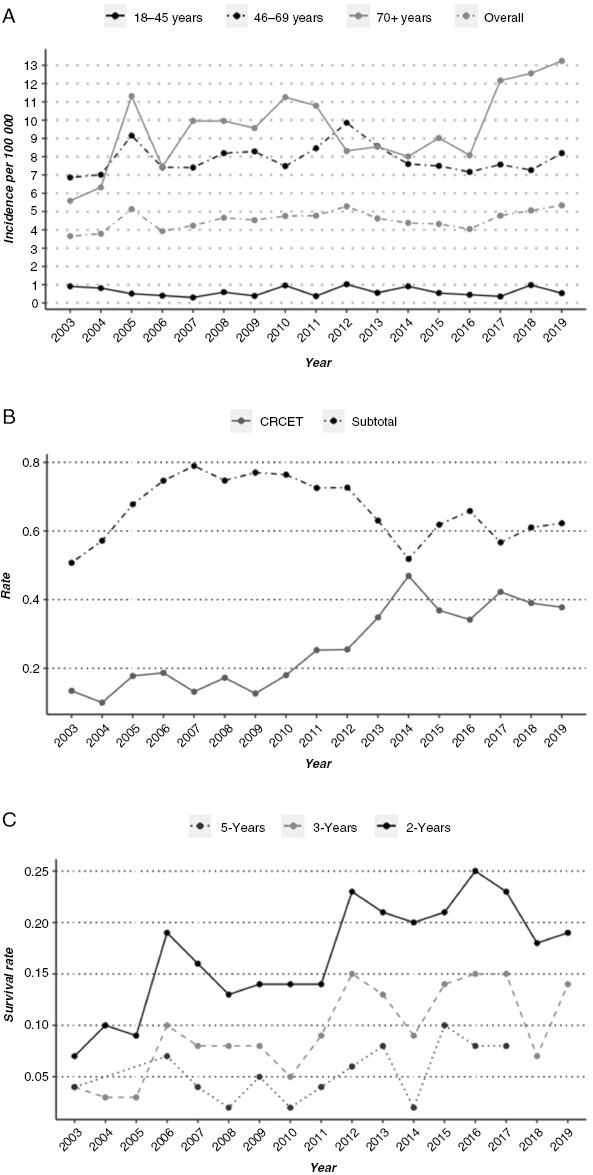
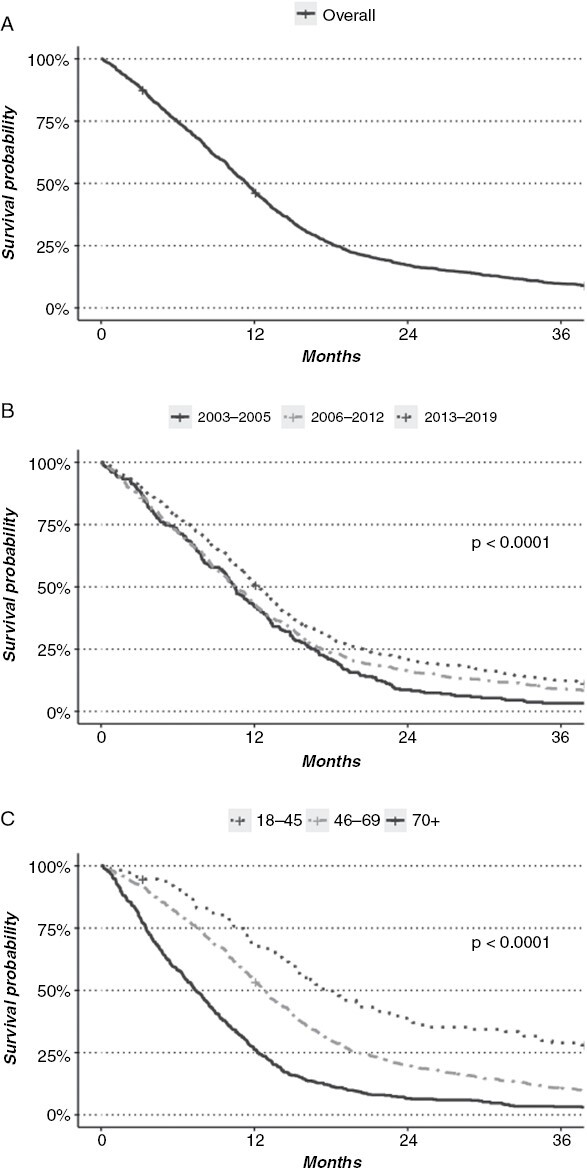
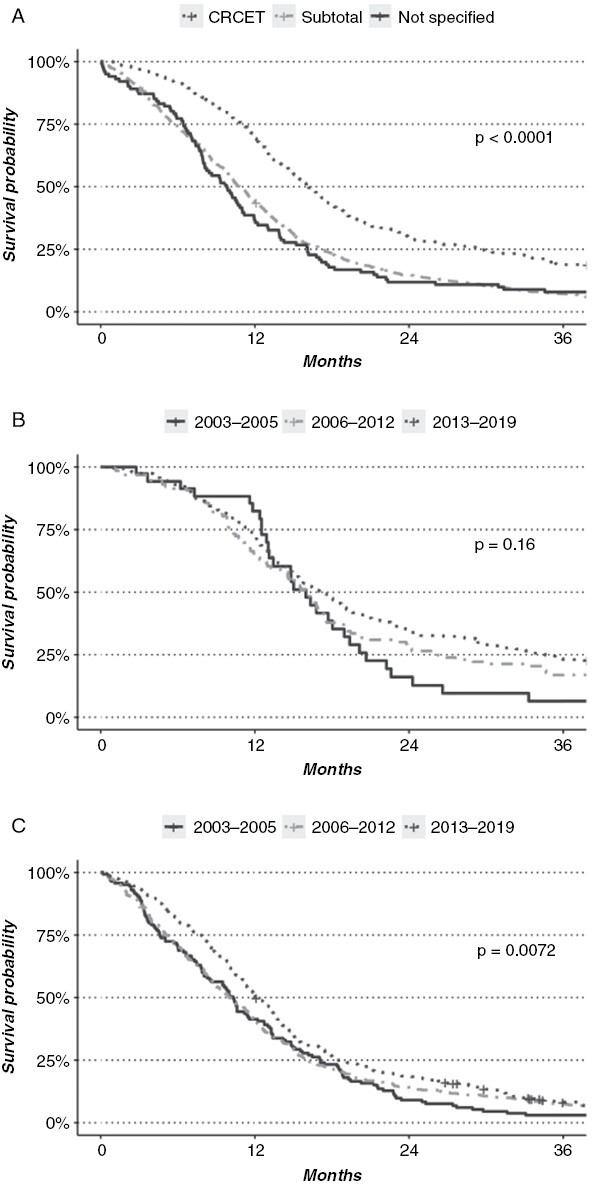
Results: The study included 1657 adult patients operated on for supratentorial glioblastoma. The incidence of histologically confirmed glioblastoma increased from 3.7 in 2003 to 5.3 per 100 000 in 2019. The median survival was 11.4 months. Complete resection of contrast-enhancing tumor (CRCET) was achieved in 386 patients, and this fraction increased from 13% to 32% across the periods. Significant improvement in median survival was found between the first 2 periods and the last (10.5 and 10.6 vs. 12.3 months; P < .01), with a significant increase in 3- and 5-year survival probability to 12% and 6% (P < .01). Patients with CRCET survived longer than patients with non-CRCET (16.1 vs. 10.8 months; P < .001). The median survival doubled in patients ≥70 years and (12.1 months). Survival was similar between the time periods in patients where CRCET was achieved.
Conclusions: We demonstrate an improved survival of GBM patients at the population level associated with an increased fraction of patients with CRCET. The data support the importance of CRCET to improve glioblastoma patient outcomes.
Keywords: complete resection of contrast enhanced tumor; extent of resection; glioblastoma; increased survival.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Conflict of interest statement
PB has received grants from The Norwegian Cancer Society South–Eastern Norway Regional Health Authority. He has received payment as a testimony expert from The Norwegian Expert Panel. He is member of the EANO guideline committee, and leader of The Norwegian Neuro-Oncology Group. EOVM has received grants from the Norwegian Cancer Society South-Eastern Norway Regional Health Authority, The Norwegian Brain Cancer Society, and The Norwegian Child Cancer Society. He has participated in the data safety monitoring board in Hemispherian AS. He has a leader role in the Norwegian Brain Tumor Consortium and the Scandinavian Society of Neurosurgery. EOVM has received payments for lectures from Regut, Norway, and Brainlab AG, Germany. PAR has received payments for lectures from Regut, Norway.
Figures
References
-
- Gzell C, Back M, Wheeler H, Bailey D, Foote M.. Radiotherapy in glioblastoma: The past, the present and the future. Clin Oncol. 2017;29(1):15–25. - PubMed
-
- Walker MD, AlexanderE, Jr, Hunt WE, et al. Evaluation of BCNU and/or radiotherapy in the treatment of anaplastic gliomas. A cooperative clinical trial. J Neurosurg. 1978;49(3):333–343. - PubMed
